

CONTENTS
Introduction.
History.
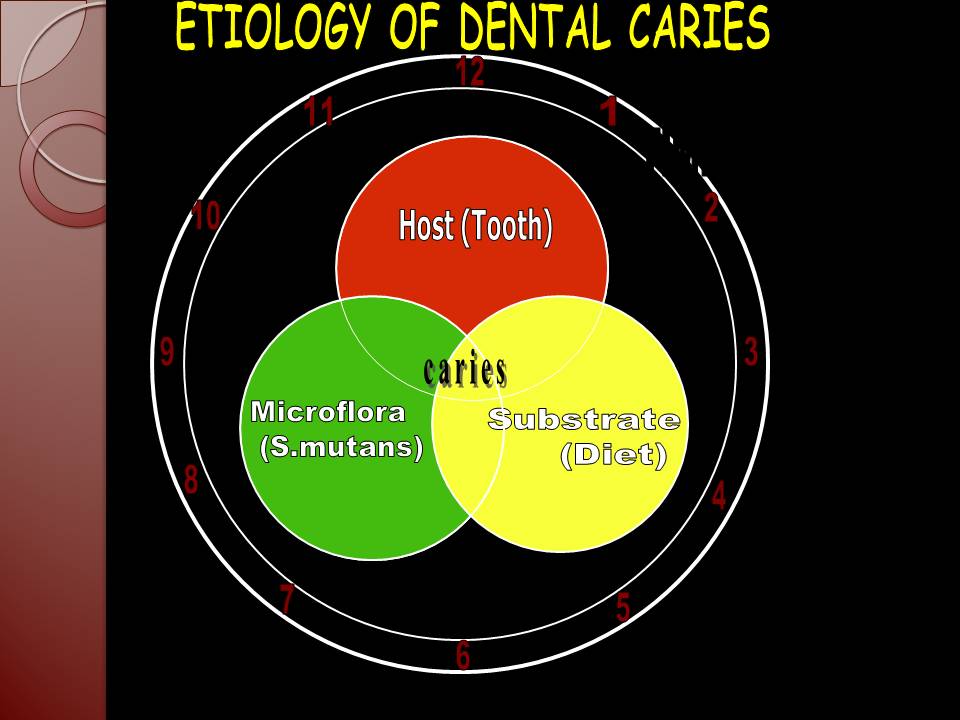
Epidemiological Triad
Methods of Dental Epidemiology.
Caries Susceptibility of : Jaw Quadrants.
Individual Tooth.
Tooth Surfaces.
Limitations of Epidemiologic
Surveys in Caries Assessment.
Economic Implications of Dental Caries.
Caries Control & Prevention.
Safeguarding Quality in Dental Epidemiologic Surveys.
Effect of Changing Dental Treatment on Epidemiology.
Summary.
Bibliography.
INTRODUCTION
EPIDEMIOLOGY:
Greek: Epi: among.
Demos: the people.
Logos: the study of.
Last’s Definition :
The study of distribution and determinants of health related states or events in the specified populations, and the application of this study to the control of health problems.
DENTAL CARIES: Latin: rot. Greek: ker- death.
Dental caries is a microbial disease of the calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth. Epidemiology: A philosophical method.
Dental Caries: A disease of modern civilization.
Challenge to epidemiologists.
Epidemiology : provides an indirect relationship between caries and etiological factors (causal inference).
By studying the Epidemiology of the dental caries……… I.Delineating the magnitude of the problem II.Recognizing the pattern of the disease III.Studying the causative factors IV. Assessing the effectiveness of the preventive measures HISTORY
A disease of modern civilization.
No caries evidence:
Pre-neolithic period (12,000 BC).
Caries evidence:
Neolithic period (12,000-3000BC).
Neanderthal Age (3000-750BC).
Pre-historic Race (15,000yrs.back). Classification of dental caries Black’s classification – Class I :
– Cavities on occlusal surface of premolars and molars.
– Cavities on Occlusal 2/3rd of facial and lingual
surfaces of molars.
– Cavities on lingual surface of maxillary incisors. Class II :
– Cavities on proximal surfaces of posterior teeth. Class III :
– Cavities on proximal surfaces of the anterior teeth
that do not involve the incisal angle. Class IV :
– Cavities on proximal surfaces of the anterior
teeth that do involve the incisal edge. Class V :
– Cavities on the gingival 3rd of facial and lingual
surface of all the teeth. Class VI :
– Cavities on the incisal edge of the anterior teeth
or occlusal cusp heights of posterior teeth. According to location on the individual teeth According to the rapidity of the process Others THEORIES OF CARIES FORMATION
I)EARLY THEORY :
The Legend of the Worm
II)ENDOGENOUS THEORIES :
a) Humoral theory
b) Vital theory
III)EXOGENOUS THEORIES :
a)Chemical (acid) theory
b)Parasitic (septic) theory
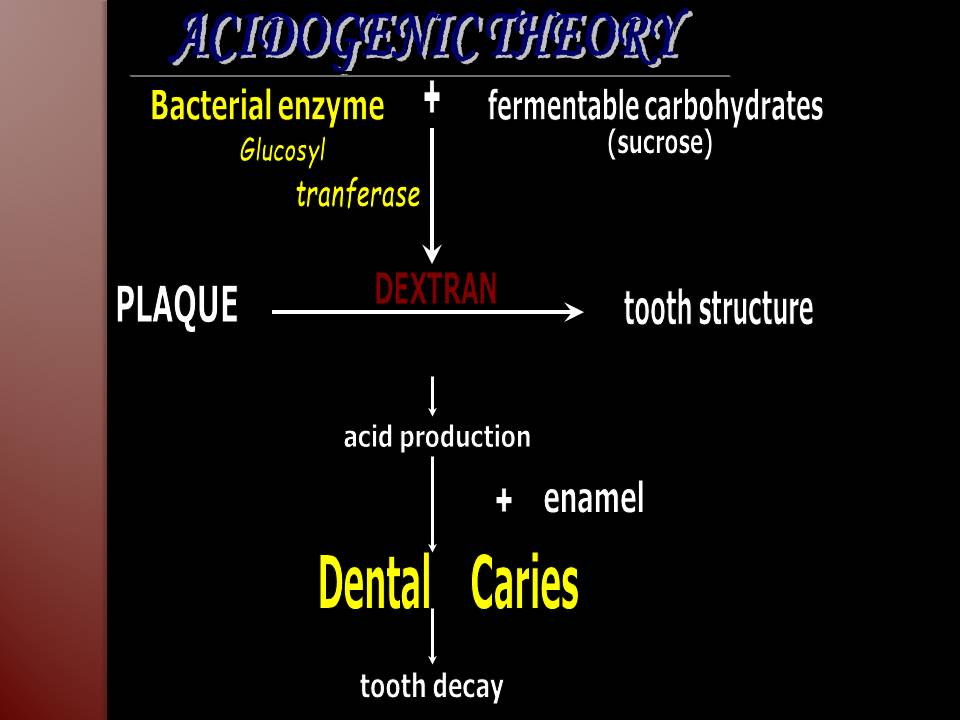
c)MILLER’S Chemicoparasitic theory (acidogenic theory) –most accepted
d)Proteolysis Theory
e) Proteolysis Chelation theory
f)Sucrose Chelation Theory
IV ) others :
a) Autoimmune theory
b)
Sulfatase theory
Etiology of dental caries
Multi-factorial
disease due to complex problems complicated by ample of indirect factors.
No universally
accepted etiology.
HOST FACTORS
AGE
Earlier it was believed that the dental caries was the
disease of the childhood and later periods of life after childhood –little
increase in the caries prevalence
But Now it is well hypothesized that the dental caries
increase—- follow certain age pattern
3 peak periods in accordance with age —- 4-8 yrs, 11-19
yrs, 55-65yrs
4-8 years
•Permanent Dentition begin to erupt and exposed to oral
environment
•Change in Dietary Habits —Sugary Snacks and sticky
food Consumption
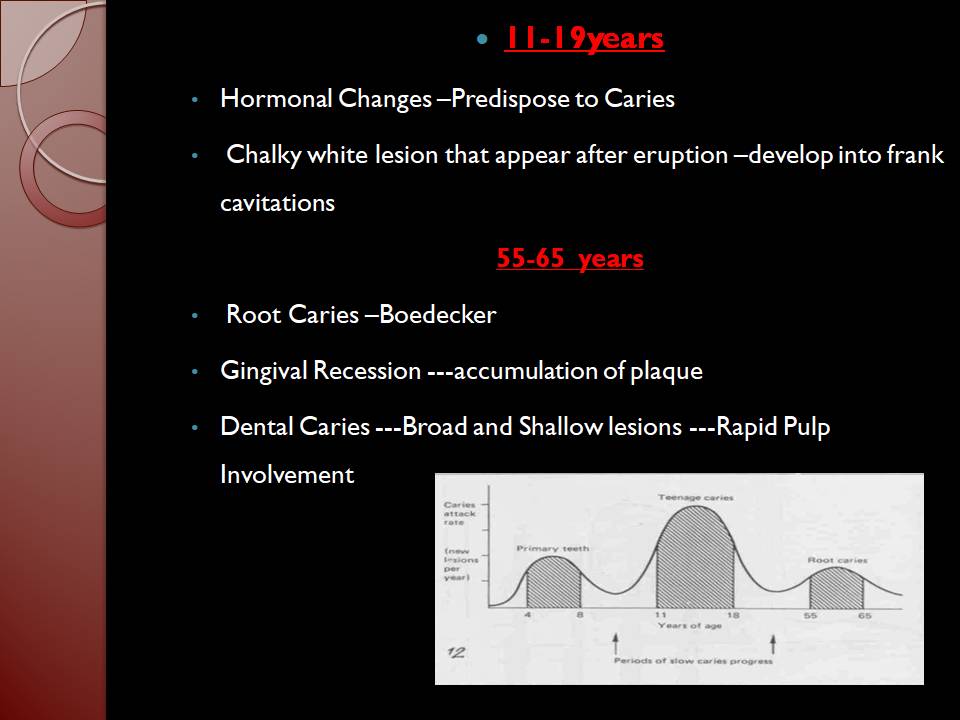
11-19years
•Hormonal Changes –Predispose to Caries
• Chalky white lesion that appear after eruption –develop
into frank cavitations
55-65 years • Root Caries –Boedecker •Gingival Recession —accumulation of plaque •Dental Caries —Broad and Shallow lesions —Rapid Pulp Involvement • SEX In the younger people dental caries have been found to be higher in the females as compared to the males(Up to age of 30 years)
Reasons Early eruption of the teeth in females as compared to the males –Prolonged exposure to the oral environment Hormonal Changes in Females —Predispose to the Caries Studies have shown that there is high caries experience in girls than boys during childhood and adolescent period. Where as some studies have shown no gender difference in later part of life. (US public health service 1967, 1987, 1988, James 1964) Whereas, Grewal H 2009, Mahesh KP 2005 and National oral health survey and fluoride mapping 2002-03, India found no gender difference in prevalence of caries in their study. RACE ¢Two factors influence the difference in caries prevalence in ethnic groups 1.Heredity 2.Environmental Influences
The classical study to establish the relation between the ethnicity and dental caries —-carried out during IInd World War Specifically it was found that caries prevalence was low in Blacks and Chinese population groups Prevalence of the Dental caries was very high in the Whites FAMILIAL HEREDITY ‘Good or bad teeth run in the family’. ¢Very few documentary evidence present linking –genetic or the heredity to dental caries ¢It has been Hypothesized there is some element of genetic predisposition to the development of the caries ¢Mans bridge et al in his study on genetics and dental caries found that the caries experience between the identical twins was similar as compared to fraternal twins EMOTIONAL DISTURBANCES Periods of stress have been associated with high caries incidence (due to decreased salivary flow). Schizophrenics experienced a reduced caries activity which may be attributed to increased salivation and higher pH of saliva (Burstone MS, 1948). A study involving 661 patients, reports close relationship between severe mental stress and dental caries (P. Sutton, 1962). Composition and Structure of Tooth Trace Elements and Dental Caries Morphology Position Variation in Individual Susceptibility of tooth to Caries
Structure and Composition of Tooth
Tooth is made up of 3 structures
Enamel
Dentin
Cementum
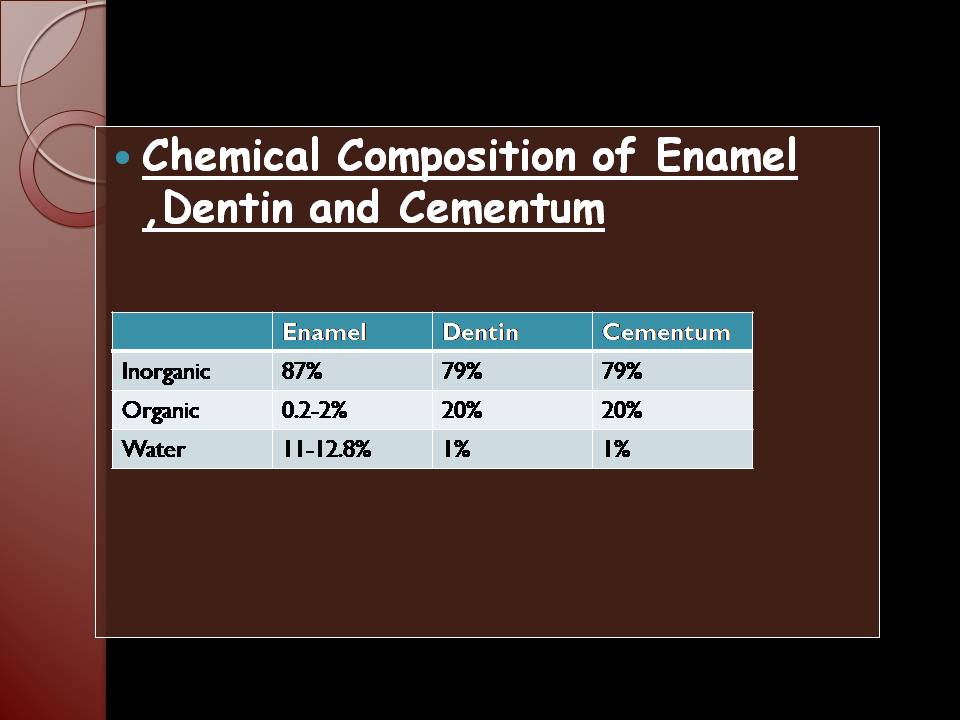
Chemical Composition of Enamel ,Dentin
and Cementum
Crystalline Structure of Tooth Enamel chiefly consists of the Hydroxyapatite mineral which is essentially made of the microcrystals of the hydroxyapatite arranged in special arrangement Morphologically crystals are rod like ,but cross section shows the Hexagonal forms Each Hydroxyapatite crystal consist of the repeating units called the unit cell Each Unit Cell is made up of 10 calcium ions,6 phosphate ions and 2 hydroxyl ions The replacement of the bipolar hydroxyl ions by the fluoride ions leads to the formation of the Fluorapatite Also some of the F ions form hydrogen bonds with the OH – ions The replacement of the hydroxyl ions by the fluorides and the formation of hydrogen bonds in some cases —-stabilizes the crystal structure of the enamel
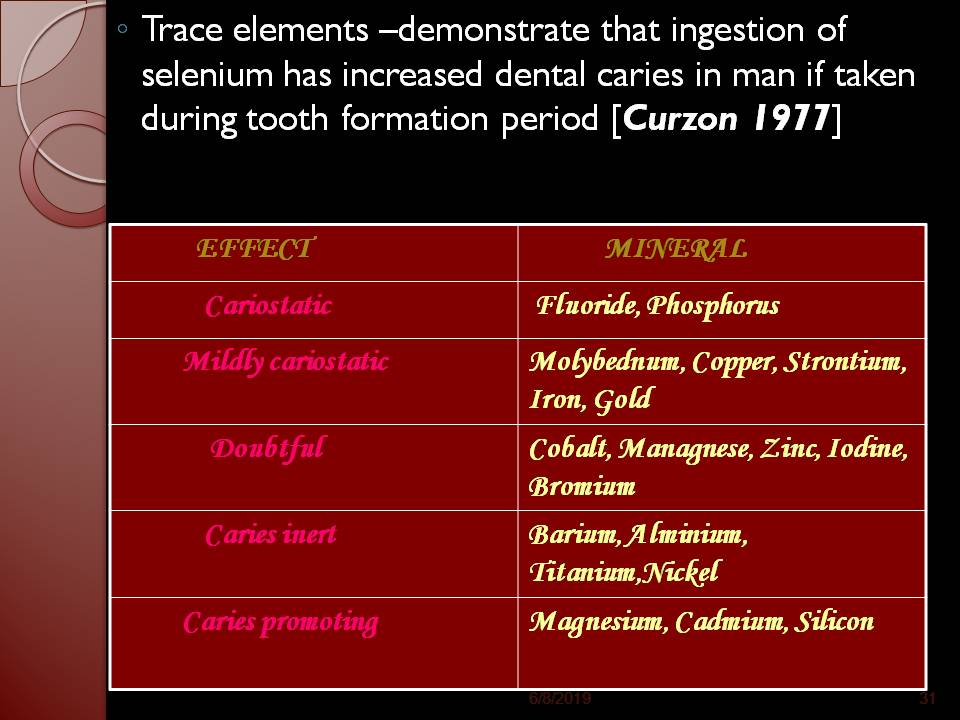
Dissolution of HydroxyApatite Crystals ¢Dissolution of the crystals in the caries is a complex process ¢Dissolution of the Hydroxyapatite crystal begins in the core and proceeds circumferentially ¢Dissolution of the Crystal depends on the four aspects of the structure and the organization of the apatite crystals 1.Lattice impurities 2.Crystal Size 3.Crystalline Defects 4.Rate of Diffusion of materials through Intercrystal Space The enamel and dentin in addition to ca and phosphate and carbonate ions –contains about 40 trace elements –most important of which are the Fluoride ions These trace element may be adsorbed to the surface of Hydoxyapatite Crystals or may replace some of the ions in the structure of apatite crystals These trace elements have important effect of the dental caries ◦Trace elements –demonstrate that ingestion of selenium has increased dental caries in man if taken during tooth formation period [Curzon 1977]
On the basis of the Morphology the teeth have 1.Pits and Fissures present on the Occlusal surface 2.Smooth Surfaces –Interproximal and Buccal The pits and fissures are more susceptible to the development of the caries than the smooth surfaces because of ¢Genetic /Inherited Predisposition of these surfaces ¢Food Retention in the deep Pits and fissures leading to the caries initiation ● POSITION- Teeth which are Malaligned, out of position, rotated or otherwise not normally situated may be difficult to cleanse and tends to favors accumulation of food and debris. Lady May Mellanby, 1934 was the first to suggest that vitamin D deficiency was the causative factor for hypoplasia and development of dental caries. In the United States, the NHANES I survey found no relation between nutritional adequacy and DMF scores W.J. Psoter 2008 among Indian children found that PEM is associated with higher caries prevalence in primary teeth but permanent teeth were not affected.
Is a broad measure of an individuals background in terms of such factors as education, income, occupation.
The first landmark research in caries epidemiology by Klien & Palmer in 1930s-1940s showed that DMF values were not uniform in different socioeconomic status groups.
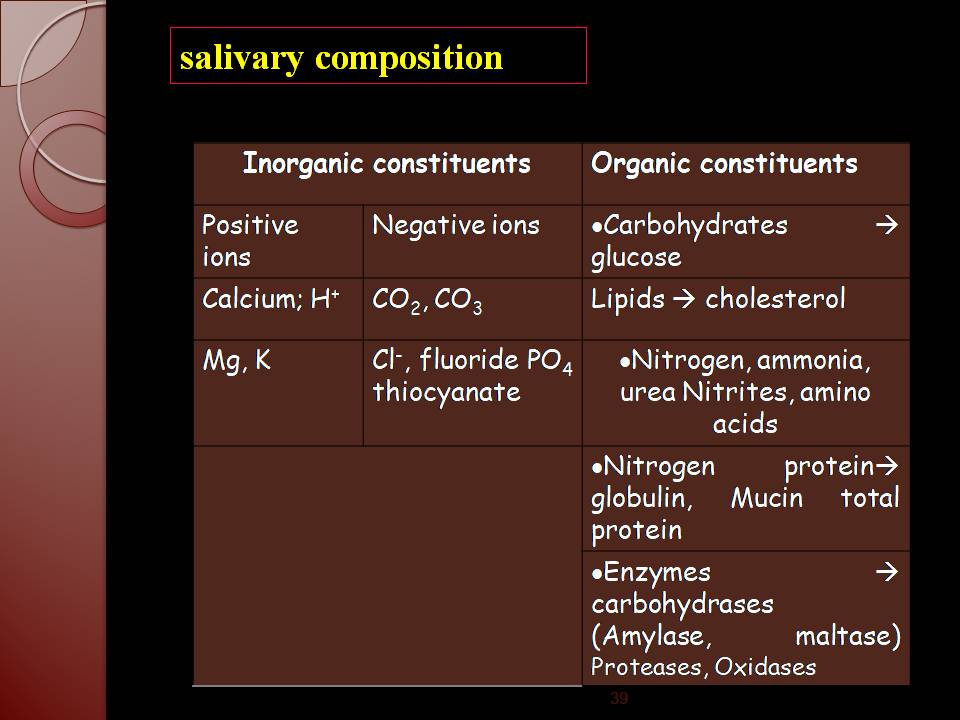
Similar results were obtained by Sogi GM 2002 and Sudha P 2005 among school children. • • Longitudinal studies (Parfitt GC, 1956) have shown that caries susceptibility rises sharply after eruption and equally falls. In general, the peak of susceptibility occurs at about 2- 4 years after eruption (Carlos JP and Gittelson1965). SALIVA Mixture of secretions of oral cavity. Its main role is in removal of bacteria and debris. Increased caries associated with xerostomia in cases of Sjogren’s syndrome, or following prolong medication with salivary depressant drugs, has been reported (Stephan RM, 1971). Rampant caries is well documented in numerous patients following radiation therapy of the mouth (Kermiol M et al 1975). salivary composition
Salivary pH Decrease in pH causes increase in caries. The PH of saliva is determined by the concentration of bicarbonates. The other factors regulating the pH of saliva are Salivary phosphates, Salivary proteins, Ammonia, Urea, and Statherin. Gopinath VK 2006 found similar results among 18-40 years old subjects.
Viscosity of saliva Miller thought that salivary viscosity was not of great importance in the caries process, since numerous cases could be found in which saliva was very viscid and the patients were free of caries. Mucin is responsible for determining the viscosity of saliva. Viscous the saliva, greater will be the risk for dental caries (Gopinath VK 2006) However further studies are needed to support this.
Buffering capacity Karshan and his associates, 1931 pointed out that the titratable alkalinity is better indication of buffer capacity than is the pH, but they found that saliva from caries free and caries susceptible persons exhibit essentially the same titratable alkalinity. In saliva chief buffer system is bicarbonate-carbonic acid (HCO3–/H2CO3) and Phosphate (HPO4 =/H2PO4 ‑). Sellman in 1949 studied the buffering capacity of saliva and its relation to dental caries and found that the total amount of acid needed to reduce the salivary pH to a given pH was always greater in saliva of caries resistant persons. Stirvick in 1950 also reported a significant inverse correlation between DMF teeth and the buffer capacity of saliva in 574 college students. Greater the buffering capacity of saliva, lesser will be the caries. (Wah Leung 1951, Eriksson 1959,1962, Abelson and Mandel 1981). AGENT ¢ ¢ ¢ ¢ ¢ MICRO ORGANISMS ¢
The classical germ free animal studies by Orland F.J et al (1954 &1955) demonstrated that – -Germ free rats on highly cariogenic diet containing sucrose did not develop caries. – -When gnotobiotic rats on the same diet were infected with combinations of an enterococcus and a proteolytic bacillus, caries developed. – –Hegde PP 2005 found that Strept. Mutans and Lactobacillus count was significantly higher among 13-15 years old with higher DMFT values in Belgaum Diet
This is the only factor that can be included under host, agent and environment factors. Physical property of food: Vipeholm study 1954 Physical nature of food: Pederson 1938 Carbohydrate content: Hopewood house study 1958 Vitamin content of the diet: SS Sidhu 1986, Nikiforuk et al 1979 Ca & p content: Gustafson et al Fluoride content:
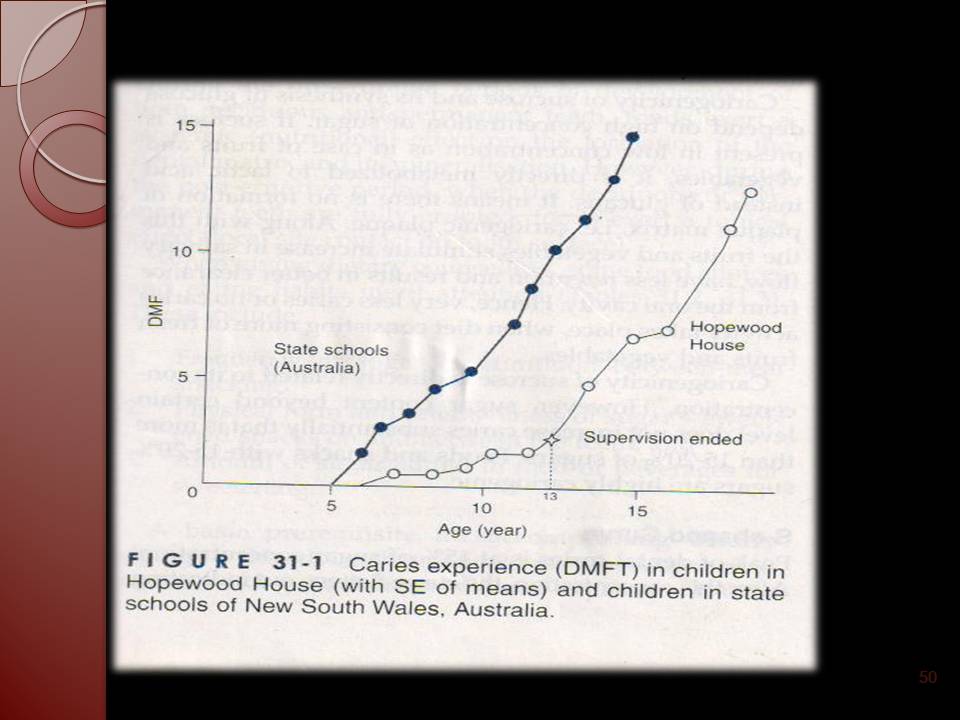
Diet: Diet refers to the customary allowance of food and drink taken by any person from day to day. The relation between the intake of refined carbohydrates, especially sugars and prevalence and severity of caries is so strong that sugars (sucrose) are clearly the major etiological factor in causation of caries. (Marthaler TM, 1968; Newbrun E, 1979 & 1982; Sucrose has been indicated as “the arch criminal” in the etiology of caries. Bowral,New South Wales, Hopewood House institution, Australia. Hopewood institution is an orphan house containing children from birth to 12 years of age. These subjects were on diet-rich in milk products and vegetables. The drinking water was having low amount of fluoride. Their oral hygiene practices were poor. Their diet mainly consisted of whole wheat, soya beans, and nuts. Cheese, sugar and refined carbohydrates were totally excluded. Observation was followed up to 13 years of age. RESULTS At the end of 10 years à 13 years old had DMFT
mean 1.6 /child General population à 13 years old mean DMFT 10.7 53% children at the hope wood house à caries free 0.4% children of state children à caries free. Hopewood house children’s oral hygiene was poor, calculus + gingivitis more prevalent in 75% of children.
Conclusion :
In institutionalized children, at least dental caries can be reduced by carbohydrate restricted diet without the beneficial effects of fluoride and in the presence of unfavorable oral hygiene.
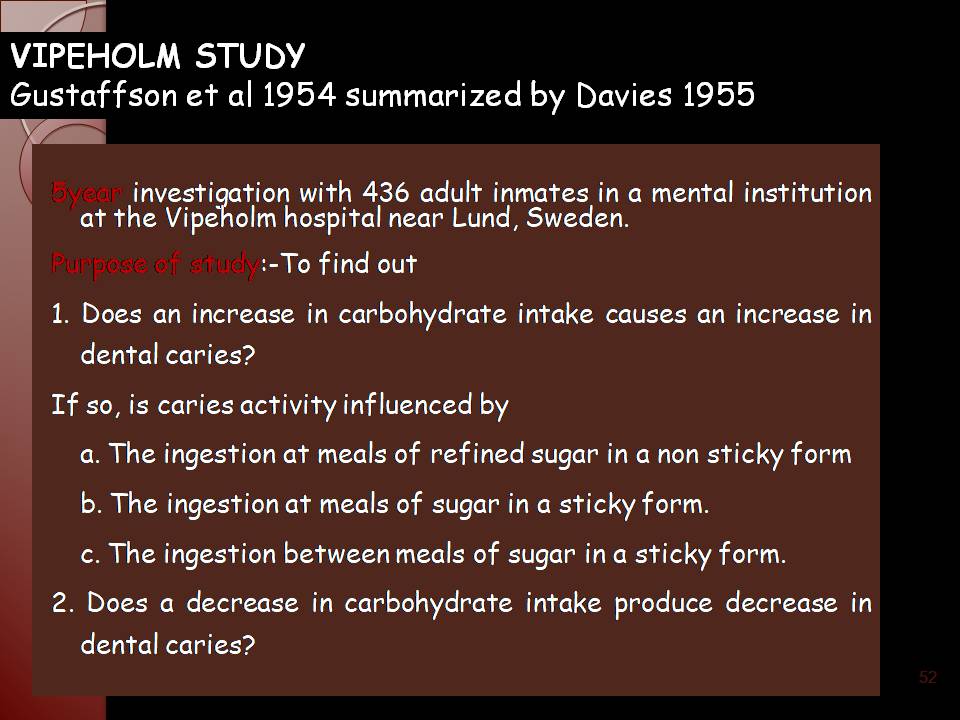
5year investigation with 436 adult inmates in a mental institution at the Vipeholm hospital near Lund, Sweden.
Purpose of study:-To find out
1. Does an increase in carbohydrate intake causes an increase in dental caries?
If so, is caries activity influenced by
a. The ingestion at meals of refined sugar in a non sticky form
b. The ingestion at meals of sugar in a sticky form.
c. The ingestion between meals of sugar in a sticky form.
2. Does a decrease in carbohydrate
intake produce decrease in dental caries?
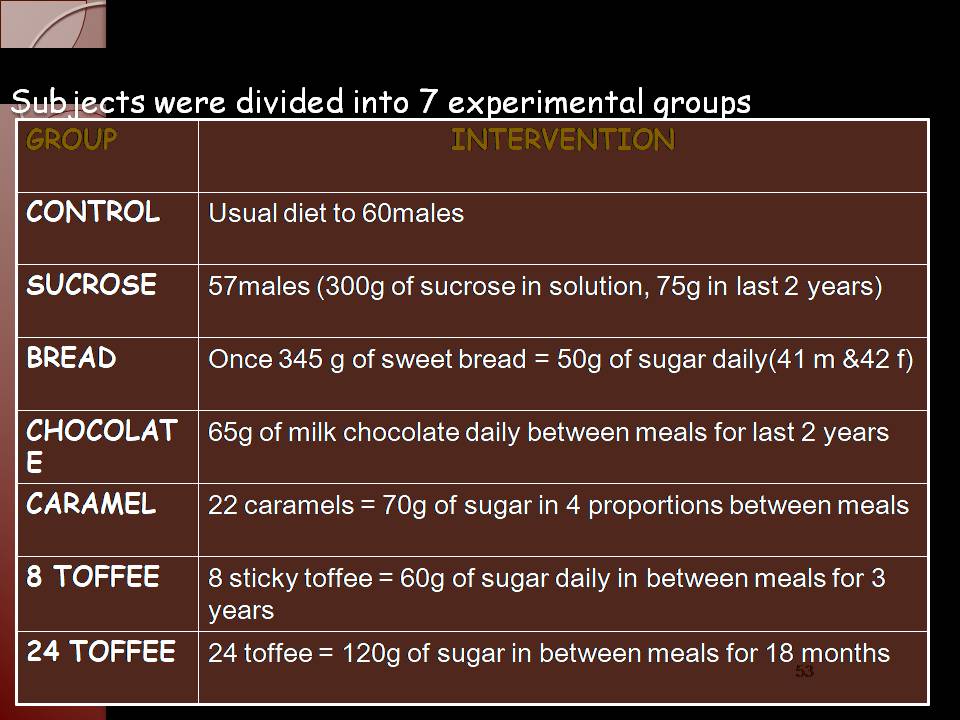
Subjects
were divided into 7 experimental groups
An increase in carbohydrate mainly sugar
definitely increase caries activity.
Risk of caries is greater if the sugar
is sticky in
nature.
The caries activity is greatest, if the
sugar is consumed between meals
Upon withdrawal of the
sugar rich foods, increase activity rapidly decrease and disappears
A high concentration of sugar in
solution and its prolonged retention on tooth surfaces leads to increase caries
activity
This study showed that the physical from of carbohydrate is much more important in Cariogenicity than the total amount of sugar ingested.
Turku study (Scheinin and Makinen, 1975)
The study investigated the effect of
almost total substitution of sucrose in a normal diet with either fructose or xylitol on caries
development.
Three groups of subjects (n = 125 in total) aged
12-53 years, sucrose: 35 fructose: 38 xylitol 52 subjects, for a period of 25
months.
Dental caries increment was monitored
at six-month
intervals by one person throughout the study and both carious cavities and
precavitation lesions were monitored.
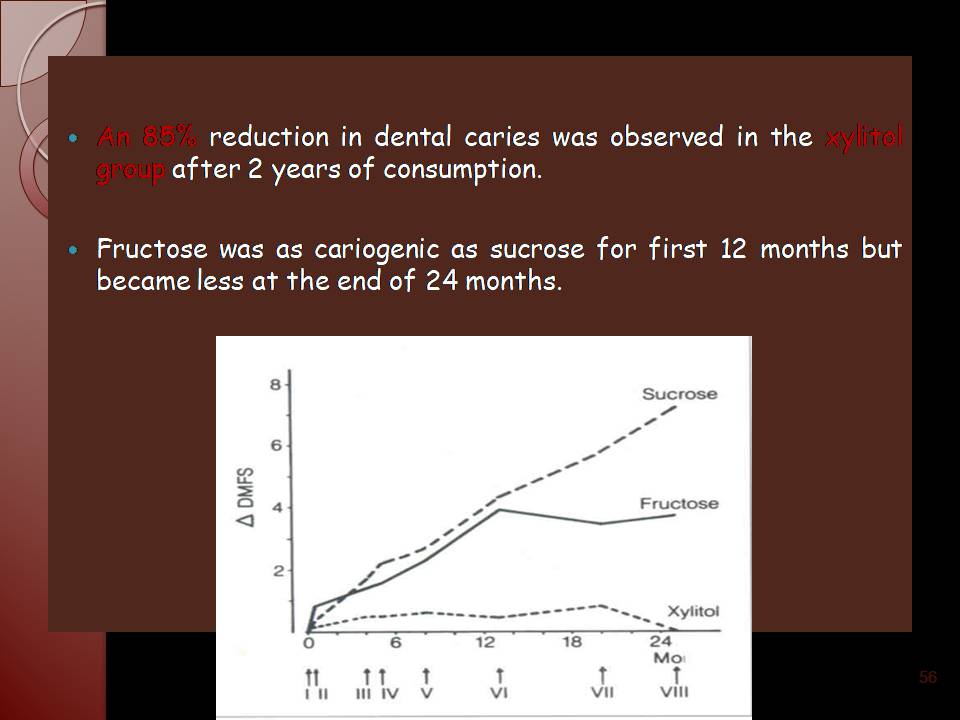
An 85% reduction in dental caries was observed
in the xylitol group after 2 years of consumption.
Fructose was as cariogenic as sucrose
for first 12 months but became less at the end of 24 months.
Hereditary Fructose Intolerance
Described by Froesch, 1959
Inborn error of fructose metabolism.
Appearance of various symptoms on
consumption of diet containing fructose or cane sugar.
Reduced level of Hepatic fructose 1
phosphate adolase with split fructose 1 phosphate to 3
carbon atom.
Reduced caries experience (Marthler, 1967).
Newbrun 1980 showed no caries experience
in Hereditary Fructose Intolerance patients compared with normal subjects.
Stephan curve (1940)
¢Stephan recorded the pH value of dental plaque in situ
before, during, and after glucose rinse.
¢
¢A typical pH response to plaque following exposure to
glucose rinse is obtained these curves are called as Stephan curve.
¢
1. Under resting conditions pH of plaque is reasonably constant, 6.9-7.2. ¢
2. following exposure to sugars the pH drops very rapidly (in few minutes) to it’s lowest level 5.5-5.2 – critical pH.
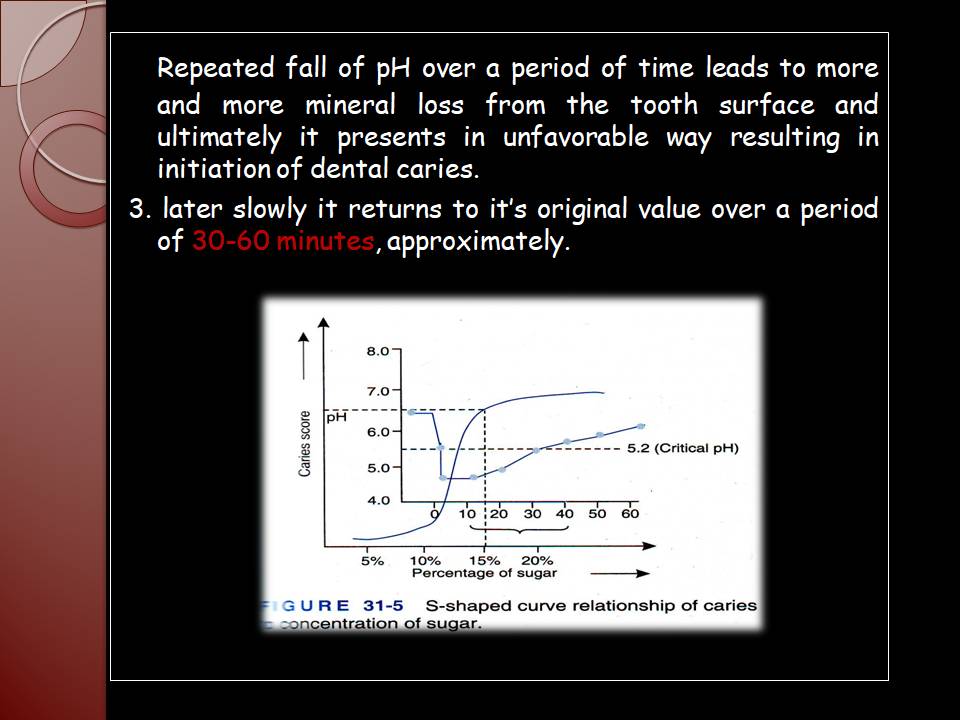
Repeated fall of pH over a period of time leads to more and more mineral loss from the tooth surface and ultimately it presents in unfavorable way resulting in initiation of dental caries.
3. later slowly it returns to it’s original value over a period of 30-60 minutes, approximately. Industrial risk Workers in the industries such as bakeries and candy factories are exposed daily to air polluted with sugar dust. Epidemiological survey of such workers has shown significantly higher caries prevalence. (15.59 ±5.97) than among workers in textile industries (9.14±4.75) (Anaise JZ, 1978). B. N. GUPTA 1990 found similar results among those working in bakery. Similarly employees in chocolate factory have been shown to have a significantly higher caries prevalence than comparable employees at a shipyard (Petersen PE 1983). Cariogenicity of sucrose Animal studies have shown that sucrose more than any other carbohydrate invariably induces the most smooth-surface types lesions. (Gustafson G et al, 1955). The principle carbohydrates available in human diets are starches, sucrose, and some lactose ; not glucose, fructose, or maltose. Phosphates and dental caries
A significant cariostatic action has been demonstrated by inorganic phosphates when added to cariogenic diets of rats or hamsters. This local effect is attributed to – ability of Phosphate ions to reduce the rate of dissolution of the hydroxyapatite of the enamel. – Lipids and dental caries Adding lipids to cariogenic diet reduces caries in animals (Bavetta LP et al, 1959; Gutafson G et al, 1953; and Rosebury T et al, 1939). Very few human studies have been done to show significant relationship. (Williams et al 1982) ENVIRONMENTAL FACTORS Geographic variation
-Latitude,
-Sunshine,
-Rainfall and
-Temperature Fluoride Trace elements Urbanization Social factors GEOGRAPHIC VARIATIONS
The three military studies best adapted to geographic analysis are those of Britten and Perrott (1941); Ferguson R.A (1935); and Nizel and Bibby (1944). The first study gives the prevalence of detectable dental defects among men who were rejected or accepted for limited duty in World War I. The second study gives the average number of decayed, missing, and filled teeth per recruit among 4,602 white naval recruits seen at one induction centre in peacetime. The third study gives average number of decayed missing teeth per selectee among 22,117 men at a large Army camp in World War II. Each of these three studies in itself show a pronounced geographic pattern for prevalence of dental disease. Latitude In the USA, the northeastern region has the highest and south-central region the lowest prevalence of caries (Klein and Palmer, 1937 and US public health service, 1988). Corroboration of this increase in dental disease with latitude is found (Mills C.A. (1937). Russell A.L. 1966 listed that the countries near the equator like India, Ethiopia, and China showed less caries compared to countries away from equator like Australia and New Zealand Distance from seacoast Caries prevalence is maximum at the seacoast and more the distance travelled away from the coastal region there will be less caries activity. Ockerse T (1949), analyzed the effect of latitude and distance from seacoast in South Africa. Andrews N.H. (1948), studied 2,000 members of the royal Australian Air Force, dividing his data by states. He found that the counts of DMF teeth vary considerably according to latitude. Sunshine Total possible hours of sunshine per year actually increase a little as near to equator (US dept. of Commerce, Weather Bureau publication no. 805, reprinted 1944), since long days in summer compensates for long nights in winter. Ultraviolet (UV) light from the sun promotes synthesis of vitamin D and along with the other factors it might account for the lower caries experience. The less the mean annual hours of sunshine high is the caries prevalence and vice a versa as shown in the studies in US and the US weather bureau map no. 13. Temperature Temperature varies with latitude and altitude. It acts to vary the caloric requirements and water intake of humans. Hence lower the temperature, higher the caries prevalence. Relative humidity Humidity shows a higher correlation with caries prevalence. Higher the humidity, more moisture in the atmosphere which block the UV rays and sunlight. Hence increased caries activity. Data from Australian states shows a higher correlation between caries and relative humidity than between caries and any other climatic factor. Bhat M 2007 found higher caries in children from fisher folk community. Rainfall Rainfall acts by leaching off minerals including fluoride from the soil and also by blocking sunlight. Rainfall and humidity are linked to dental caries prevalence, either separately or together. Fluoride Higher the fluoride content in the soil and ground water, lesser the caries. The maximum caries reduction is noticed at the level of 1 ppm of fluoride from all sources- from water, soil, atmosphere, food etc. Van Burkalow’s mapping (1946), of maximum fluoride concentration in communal and non communal water supplies on a country basis gives the most comprehensive material available for united states. Total water hardness Water hardness is measured by the concentration of calcium carbonate. An inverse relation is seen between caries and water hardness. Rose C; 1909; Mills C.A. 1937 and Ockerse T. 1949, are among the authors who have reported an inverse relationship. Soils Soil composition bears an influence on caries, where populations consume largely locally grown foodstuffs. Children in Napier, who consumed locally grown food containing a higher molybdenum and also higher pH, resulting in low caries prevalence. Ludwig, Healy, and Malthus (1962- Newzealand), noted marked difference in caries between the towns of Napier and Hastings, without any environmental factor other than soil to account for it. Urbanization Furguson R.A. (1935), attributed the regional variations he found in caries to the greater frequency of large industrial cities in the North America. Rao SP 1993 found that dental caries were more prevalent among urban children than rural and tribal children. Similar results were obtained by Vinit Dhar 2009 among children of Udaipur city Nutrition Nutrition can also be included under environmental factors as geographic (soil, temperature), cultural or educational factors, which might influence food availability and, in turn, might contribute either for increase or decrease in caries activity. e.g. previously Eskimos diet included only animal fat from fish and seals (proteins and fats). The results have been excellent for the Eskimos dentition, as the work of Waugh L.M. (1931) and others testifies. Social factors Like economic status, social pressure, affordability, provision of good preventive measures etc. might create more demand for better dental care and leads to lesser caries prevalence. Sogi GM 2002 and Sudha P 2005 showed that social factors has a influence on prevalence of dental caries. ¢The term pandemic is customarily reserved for global disease outbreaks that are acute and fatal, suggests an impact on populations of entire countries, continents, or much of the world. ¢The term therefore implies two elements: global distribution and severe consequence ¢By this definition dental caries can be characterized as a pandemic—Global Distribution and profound severity and societal significance The World Health Organization’s 2003 report on oral health provides an overview of global caries epidemiology Globally, WHO reports caries prevalence in school age children at 60–90% and as virtually universal among adults in the majority of countries ¢Global overview of changes in dental caries levels focuses on 12-year-olds, since they are the most commonly studied age group for the purposes of comparative dental epidemiology Most industrialized countries and some countries of Latin America show high DMFT values (i.e. 14 teeth or more) Levels of dental caries experience are much lower in the developing countries of Africa and Asia. In several industrialized countries, older people have often had their teeth extracted early in life because of pain or discomfort, leading to reduced quality of life
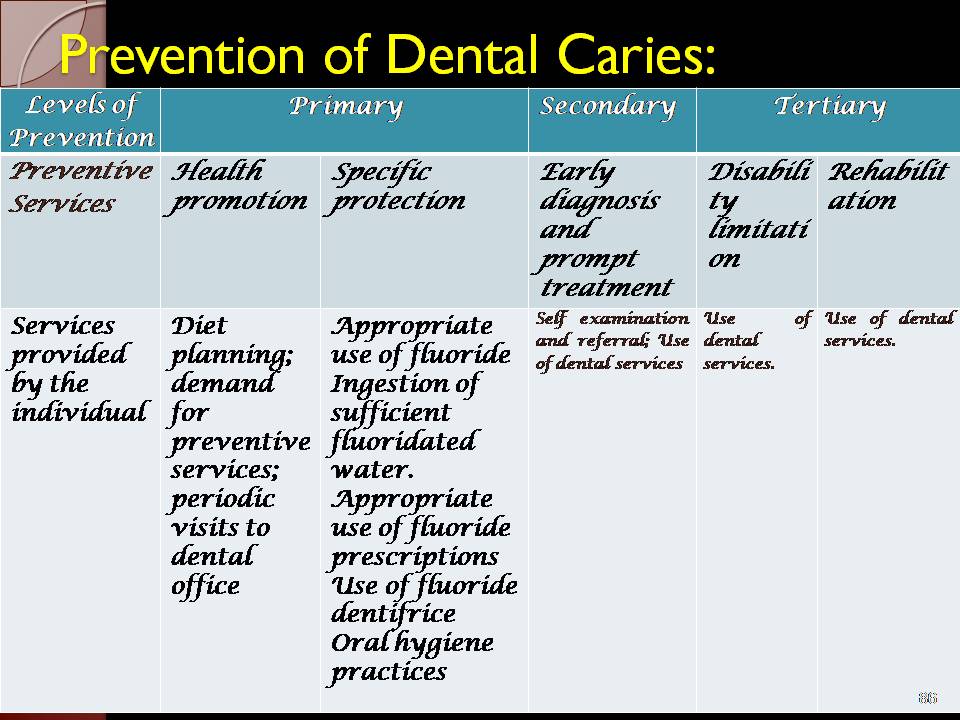
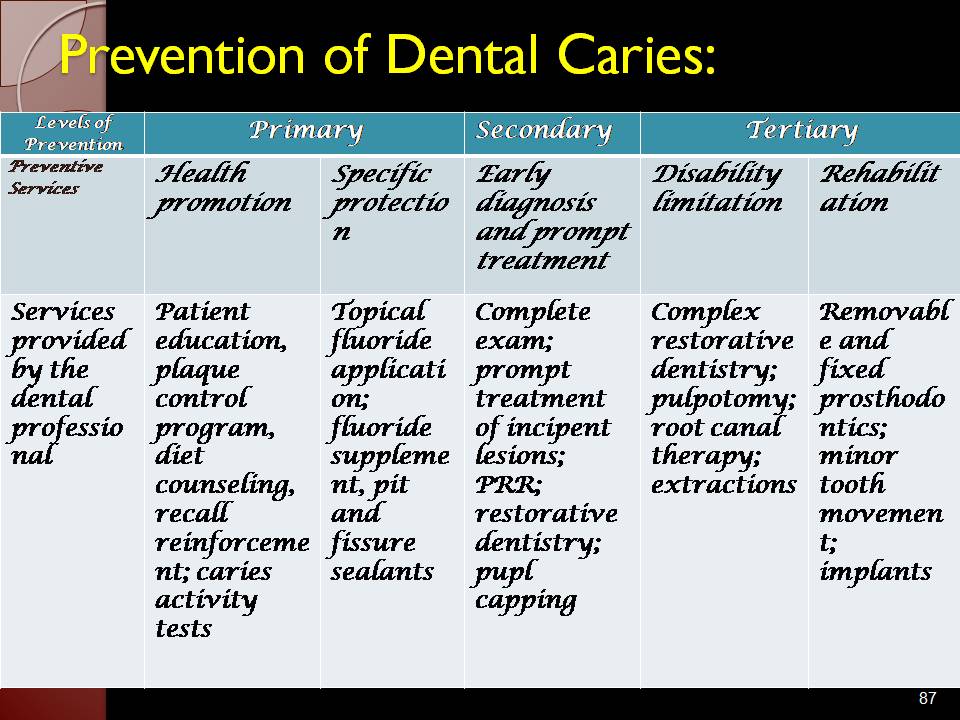
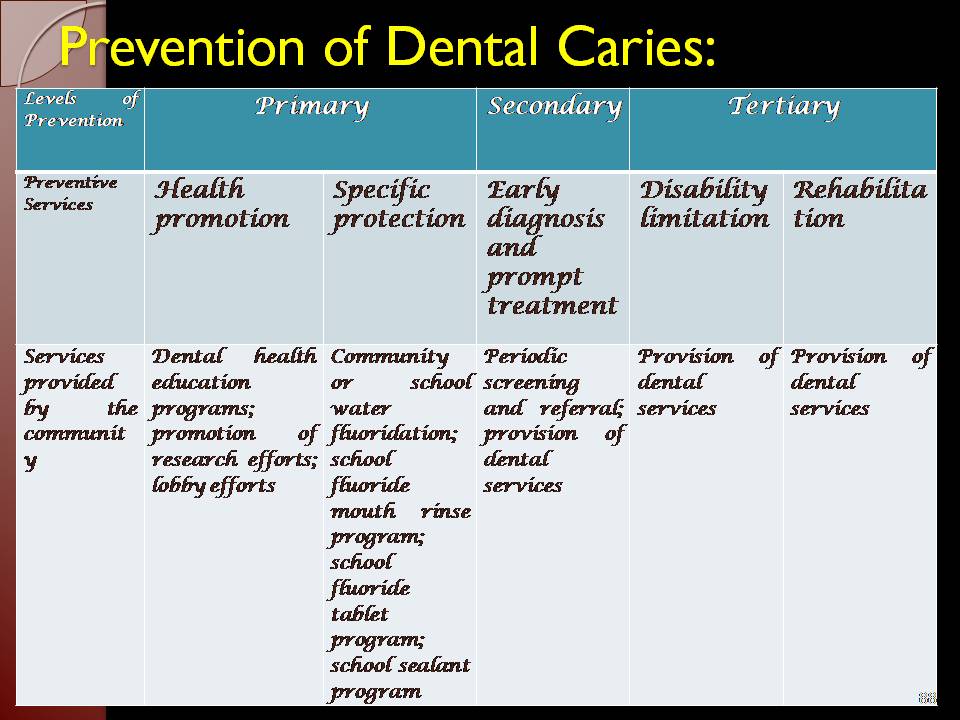
Caries prevention is based up on attempts:
1. Increase the resistance of the host (fluoride therapy, occlusal sealants, immunization).
2. Lower the number of micro organisms in contact with tooth (plaque control),
3. Modify the substrate by selecting non – cariogenic food stuff and
4. Reduce the time that the substrate is in the mouth by limiting the frequency of intake. CARIES CONTROL & PREVENTION 1.Educate early:
Start with expecting mothers:
a.) Primary teeth: 2months gestation.
Permanent teeth: 6months gestation.
Early mal-nutrition:
delayed tooth eruption. decreased strength.
increased caries. decreased resistance in kids.
b) Explain primary factors and acid production.
2. Increase tooth resistance and reduce microbial challenge:
Brushing.
Chemical agent: chlorhexidin.
Use of floss.
Fluoride application.
Diet modification. Prevention of Dental Caries: Prevention of Dental Caries: Prevention of Dental Caries: SUMMARY Epidemiologic measures are concerned with populations rather than individuals, hence, constitutes the basic science of public health. The balance between dental health and dental caries is delicate. With a change in caries progression & lesion morphology, there comes a change in epidemiologic measures.
Hence, dental caries poses new challenges to epidemiologists. Today, the most common epidemiological measure (WHO) in caries assessment is: DMFT(S).
The prevalent criteria tends to under-estimate actual caries prevalence.
Hence, there is need for development of improved caries- diagnosis and assessment procedures in order to plan and execute better public health programmes for promotion of global oral health.
Against the standard visuo-tactile method of caries diagnosis, WHO is expected to shift to use visual method in epidemiological surveys in the near future.
There has been introduction of SIGNIFICANT CARIES INDEX (SiC Index) that focuses on ‘maximum caries-exposed individuals’ rather than prevalent ‘ number of caries exposed individuals.’
It has yet to be brought into practice.
Dental caries is still a considerable burden largely in Developing and still in Developed countries.
Foregoing through dynamics of epidemiology of dental caries, which has been primarily descriptive, is indicative of variety of causative factors for Dental caries.
Data pertaining to various trends in dental caries is still lacking in India.
Further exploration using epidemiology as a tool for probing the causal factors operating in our country will certainly throw a light in understanding and management of dental caries 1.Burt BA, Eklund SA. Dentisty, Dental Practice and the Community. 6th ed, Elsevier, 2005. 2.Dunning JM. Principles of Dental Public Health. 4th ed. Harvard University Press. Page 476-500. 3. Marya CM. A Textbook of Public Health Dentistry. 1st edition. India: Jaypee; 2011. 4.Abdul Arif Khan, Sudhir K. Jain, and Archana Shrivastava. Prevalence of Dental Caries among the Population of Gwalior (India) in Relation of Different Associated Factors. Eur J Dent. 2008 April; 2: 81–85. 5.Psoter W. Effect of early childhood malnutrition on tooth eruption in Haitian adolescents. Community Dent Oral Epidemiol. 2008 Apr;36(2):179-89. ● ● ● 6.Sudha P. Prevalence of dental caries among 5-13 years old children of Manglore city. J Ind Soc Pedod Prev Dent 2005 74-77. ● 7.UM Das, JP Beena, U Azher. Oral health status of 6- and 12-year-old school going children in Bangalore city: An epidemiological study. J Ind Soc Pedod Prev Soc 2009;27 : 6-8. ● 8.Hegde PP. Dental caries experience and salivary level of streptococcus and lactobacillus in 13-15 yaers children of Belagaum city, Karnataka. 2005: 23-27. ● 9.Hiremath SS. Textbook of Preventive and community dentistry.2nd edition, India: elsevier;2007 ● 10.Peter S. Essentials of Preventive and Community dentistry,4th edition, New Delhi, India: Arya publishing House;2010
11. Kenkre, A M, Spadigam, A E. Oral health and treatment needs in institutionalized psychiatric patients in India. Indian Journal of Dental Research. 2000 Jan-Mar; 11(1): 5-11.
12. Sumati Bhalla, Shobha Tandon, K Satyamoorthy. Salivary proteins and early childhood caries: A gel electrophoretic analysis. Contemp Clin Dent 2010;1:17-22
13. Vineet Dhar, Maheep Bhatnagar. Dental caries and treatment needs of children (6-10 years) in rural Udaipur, Rajasthan. J Ind Soc Pedod Prev Dent 2009; 20: 256-260.
14. Joseph Z. Anaise. Prevalence of dental caries among workers in the sweets industry in Israel. Community Dentistry and Oral Epidemiology. 1978; 6: 286–289.
15. National Oral Health Survey and Fluoride Mapping 2003 :DCI

Leave a comment