
CONTENTS
- Introduction
- Personal information
- Taking and recording history
.Chief complaint .History of present illness
.Past dental history .Past medical history
.Personnel history .Family history
- Examination of the patients
.General examination
.Extra-oral examination
.Intra-oral examination
Soft tissue
Hard tissue
- Establishing the diagnosis
.Provisional diagnosis
.Differential diagnosis
.Laboratory investigations
.Final diagnosis
- Treatment planning
- Conclusion
INTRODUCTION
History taking is an art which a doctor learns by repeated practice and experience.
A kind and considerable approach is most important in securing and gaining confidence of the patient.
A friendly atmosphere is an important factor in helping patient to talk freely about his problems.
Case History – defined as a planned, professional conversation that enables the patient to communicate their symptoms, feeling and fears to the clinician so that the nature of patient’s real and suspected illness and mental attitudes may be determined.
PERSONNEL INFORMATION
NAME:
A patient usually likes to be called by their name.
In case of pediatric patients, it encourages him/her to talk freely.
AGE:
Certain diseases are more common at certain ages.
1) Diseases present at/since birth:
for eg. – Facial hemihypertrophy, cleft lip, cleft palate, etc.
2) Diseases frequently seen in children and young adults
for eg. – Juvenile periodontitis, torus palatinus, basal cell
carcinoma, sickle cell anemia, etc.
3) Diseases frequently seen in adults and older patients
for eg. – Attrition, abrasion, gingival recession, periodontitis,
pernicious and iron deficiency anemia, diabetes,
hypertension, etc.
SEX:
Certain diseases are more common in a certain sex
1) Diseases more common in females:
Iron deficiency and sickle cell anemia, thyroid diseases, juvenile periodontitis, recurrent apthous stomatitis, idiopathic thrombocytopenic purpura, etc.
2) Diseases more common in males:
Attrition, carcinoma of the buccal mucosa, leukoplakia, herpes simplex, multiple myeloma, osteoblastoma, basal cell carcinoma, etc.
OCCUPATION:
Some diseases are peculiar to certain occupations:
Attrition – certain workers exposed to an atmosphere of abrasive dust or the habitual
opening of the pins may result in notching of the incisal edge.
Abrasion – commonly noticed in carpenters, shoemakers or tailors who hold pins, nails or
tacks between their teeth.
Erosion – undue erosion is seen in sand-blasters.
Gingival staining – strange dark stippling of the marginal gingiva is seen in lead, bismuth
or cadmium workers.
Hepatitis-B – dentists, general surgeons, blood bank personals, etc. are very prone to it.
ADDRESS:
It is necessary for future correspondence.
Full postal address should be taken for future communication.
Certain diseases prevail more in certain geographical areas.
Dental caries and mottled enamel are dependent on the fluoride content of the domestic water.
In India, cancer of lip is rare whereas cancer of tongue and buccal mucosa constitutes the bulk of oral cancers.
Dental caries is more common in modern industrialized areas while periodontal diseases are more common in rural areas.
RELIGION:
Certain diseases are more common in a certain religions.
Carcinoma of penis is hardily seen in Jews and Muslims owing to their religious custom of compulsory circumcisions of penis.
On the hand, intussusceptions are sometimes seen after the month long fast in Ramjan in Muslims.
TAKING AND RECORDING HISTORY
Basic principles of history taking:
- Introduce your self and greet the patient by name
- Put patients at their ease
- Start with the open questions
- Mix open and close questions
- Avoid leading questions
- Avoid jargon
- Asses patients mental state
- Asses patients expectations from treatment
Significance of history taking:
- To get better rapport with the patient
- To gain confidence of the patient
- To asses the mental and emotional state so that patients psycho-somatic diseases can be observed.
CHIEF COMPLAINT:
It is the reason for which patient has came to doctor or the reason for seeking treatment.
Chief complaint should be recorded in patients own words and in a chronological order.
If few complaints start simultaneously, record them in order of severity.
Chief complaint aids in the diagnosis and treatment planning.
While noting complaint, one should be precise for its duration and the onset.
Most common chief complaints are pain, burning sensation, bleeding gums, loosening of teeth, decayed teeth, swelling, and halitosis.
HISTROY OF PRESENT ILLNESS:
It is the chronological account of the chief complaint/s and associated symptoms from the time of onset to the time the history is taken.
Elaboration of chief complaint in detail:
It includes
Mode of onset – sudden or gradual and duration.
Cause of onset – the thing that precipitated the signs and symptoms.
Progress of pain – nature of pain, intensity of pain, Aggravating and relieving factors.
Relapse and remission
Treatment – if the patient has taken any treatment for the same problem.
PAST DENTAL HISTORY:
It provides an idea about the attitude and awareness of the patient towards dental care, any complication associated with previous dental treatment such as excessive bleeding after extraction or any allergic reaction or any fainting episode.
PAST MEDICAL HISTROY:
Diabetes Mellitus
Cardiac Problems
Respiratory Diseases – Asthma
Drug Allergy
Neurological Disorders – Epilepsy
History of recent hospitalization
Radiotherapy to the head or neck region in the recent past.
Blood transfusion in the recent past.
Immunological diseases – AIDS.
Pregnancy in case of female patients.
PERSONEL AND SOCIAL HISTROY:
Habits: Oral hygiene and brushing technique
Improper oral hygiene and brushing causes dental caries and
Periodontal diseases.
Horizontal brushing causes cervical abrasion of teeth
Pressure habits: Lip sucking, Thumb sucking, and finger sucking leads to proclination of maxillary anterior teeth.
Tongue thrusting: Anterior and posterior open bite
Mouth breathing: Anterior marginal gingivitis and caries
Bruxism: Lead to attrition
Patient’s appetite:
Regular/ Irregular
Type of diet: Soft diet causes caries as it sticks to teeth than coarse diet
Increased carbohydrate diet causes caries where as phosphates diets prevent caries.
Diets deficient in vitamins causes enamel hypoplasia during embryogenesis.
Sleep
Adverse habits:
Tobacco: Pan Masala, Gutkha.
Alcohol (quality and quantity)
Smoking (cigarettes, cigar/ pipe) — Frequency duration.
Women: Menstrual history.
FAMILY HISTROY:
Many diseases recur in families like:
Hemophilia
Diabetes Mellitus
Hypertension
Heart Diseases
General examination:
1. Vital signs:
a. Pulse: important index of severity of illness, abnormalities of heart and vascular system. E.g. hypertension, hypotension, shock, fever.
Pulse rate: Slow or fast (normal: 60-100 beats/min)
Pulse rhythm: Regular/Irregular
E.g. irregularly irregular in atrial fibrillation
Regularly irregular in ventricular failure.
Pulse volume: High, low and normal
Indicates pulse pressure (40-60 mmHg)
Narrow pulse pressure — LVF, MS, AS.
Wide pulse pressure: Aortic and mitral regurgitation
High output states like pregnancy and anemia.
Tension and force: Indicates SBP and DBP
Character: E.g. water hammer pulse: AR
Pulses paradoxes: Pericardial effusion
Anerotic pulse: AS
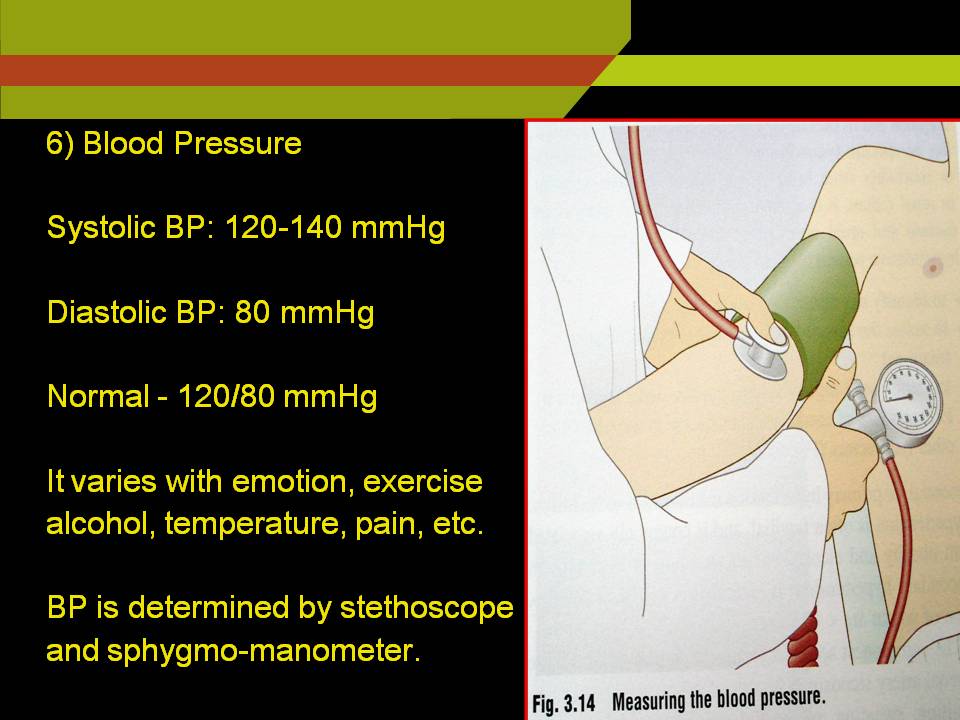
Blood pressure:
SBP: 120-140 mmHg
DBP: 80 mmHg 120/80 mmHg
BP varies with emotion, exercise, meal, alcohol, tobacco, temperature and pain.
Increased BP- Hypertension
Decreased BP- Hypotension
Equipment:
Stethoscope and Sphygmomanometer
Procedure:
Ask the patient to seat and place his right arm on a table so that the forearm is adequately supported at the elbow level above the level of heart.
Center the rubber balloon of the cuff over the brachial artery
Wrap the pressure cuff smoothly and snugly around the upper arm with its lower border 1-2 inches above the elbow crease in the antecubital fossa.
Palpate the patient radial pulse and pump the cuff up to above 20-30 mmHg the point at which the pulse is no longer palpable.
SBP always recorded by palpation to avoid missing the occasional occurrence of silent gap in hypertensive patients.
Apply either bell/ diaphragm of the stethoscope over the artery and slowly deflate the cuff about 3mmHg/heart beat until first sound appears which is recorded as SBP.
Lower the pressure in the cuff until the sound disappears record this point as DBP.
Faulty technique in taking BP may induce error,
If cuff applied too loosely if it is not completely deflated before applying.
Anxiety and pain may elevate BP of the patient above his true resting level.
Temperature:
Normally taken in the mouth or in the axilla by keeping mercury thermometer for a minute.
Temperature of mouth is about 1 degree higher than that of axilla
Normal body temperature varies from 36-37.5c lowest temperature between 2 – 4 am and highest in the afternoon.
Normal oral temperature is 37c
Rise in temperature above normal is FEVER
TYPES:
1. Continuous fever: temperature remains above the normal through out does not fluctuate >1c in 24 hours.
E.g. Typhoid, Lobar pneumonia.
2. Remittent fever: temperature remains above the normal through out the day fluctuates >1c in 24 hours.
3. Intermittent fever: temperature is present only for some hours in a day and remits to normal for the remaining hours. E.g. Malaria, Septicemia.
Respiration:
Normal rate 14 to 18 cycles/min
Tachypnea (fast breathing): Fever, shock, hypoxia, tetany, metabolic acidosis.
Bradypnea: slow and deep respiration seen in cerebral compression.
General physical examination:
- Built and gait of the patient:
Built; skeletal structure in the relation to age and sex of the individual as compared to normal person
Gait; the way patient walks
Well
Moderate
Mild
- Pallor, cyanosis, clubbing, icterus, lymphadenopathy, and edema.
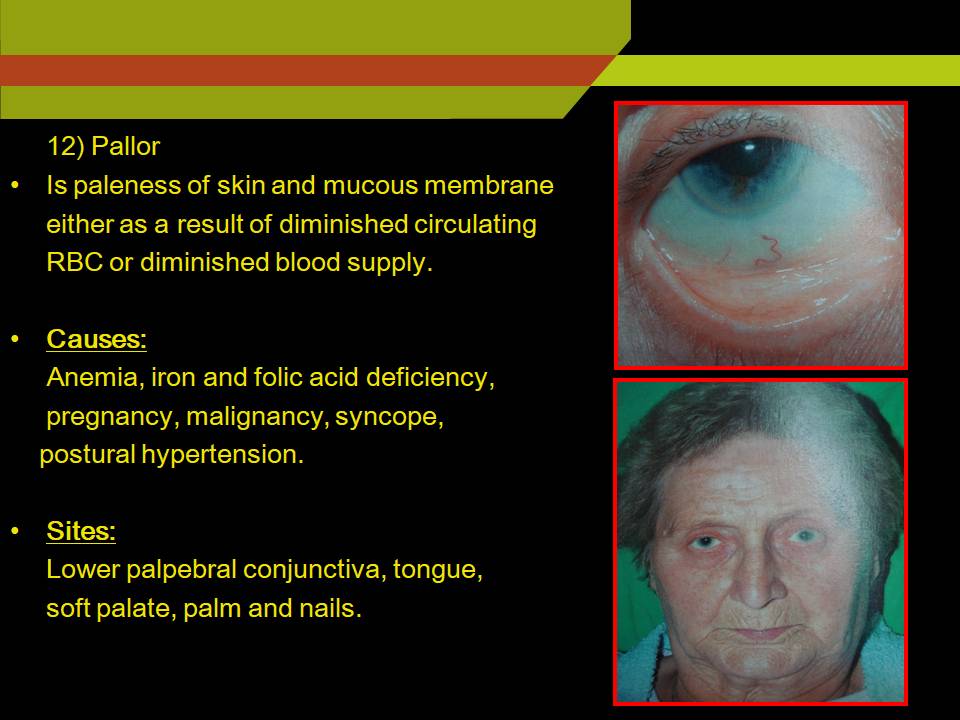
PALLOR:
Is paleness of skin and mucous membrane either as a result diminished circulating RBC or diminished blood supply
Causes:
a. Anemia
Hemorrhagic
Hemolytic
Dyshemopoietic
Decrease iron, folic acid, vitamin B12
Pregnancy
Malignancy
Syncope
Postural hypertension
Arterial occlusion
Sites: lower palapebral conjunctiva, tongue, soft palate, palm and nails.
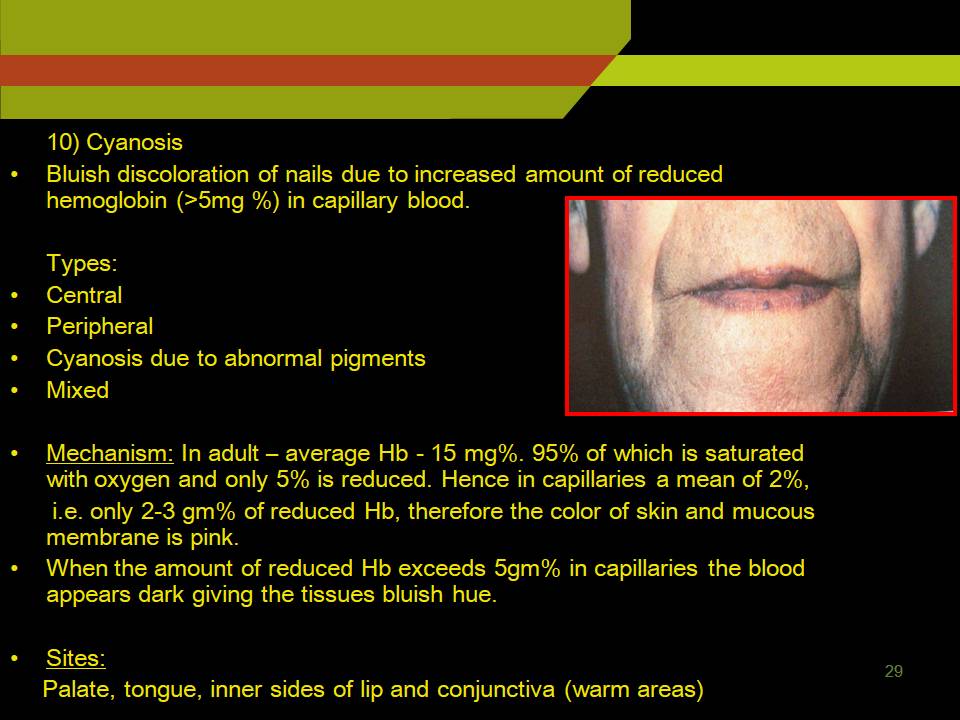
CYANOSIS:
Bluish discoloration of nails due to increased amount of reduced hemoglobin (>5mg %) in capillary blood.
Types:
Central
Peripheral
Cyanosis due to abnormal pigments
Mixed
Mechanism: Adult on an average there is 15 mg % of Hb, 95% of which is saturated with oxygen and only 5% is reduced. Hence in capillaries a mean of two i.e. only 2-3 gm% of reduced Hb and color of skin and mucous membrane is pink.
When the amount of reduced Hb exceeds 5gm% in capillaries the blood appears dark giving the tissues bluish hue.
Sites:
Palate, Tongue, Inner sides of lip and conjunctiva (warm areas)
Causes:
1. Central:
a. Cardiac: Congenital, cyanotic heart disease, fallots tetrad.
Congenital cardiac failure
b. Pulmonary: Chronic obstructive lung disease
Collapse and fibrosis of the lung.
- High altitude due to low partial pressure of oxygen
2. Peripheral:
Cold
Increased viscosity of blood
Shock
3. Mixed; Acute left ventricular failure, Mitral stenosis.
Cyanosis due to abnormal pigments:
Methemoglobinemia
Sulfhemoglobin
Cyanosis does not occur: In severe anemia
Carbon monoxide poisoning.
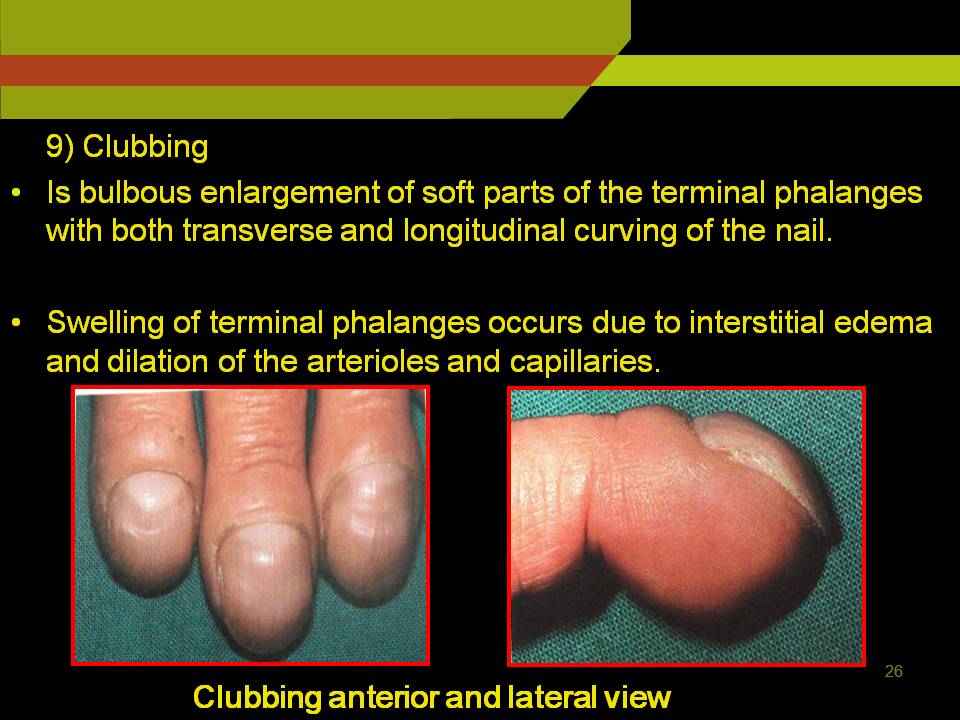
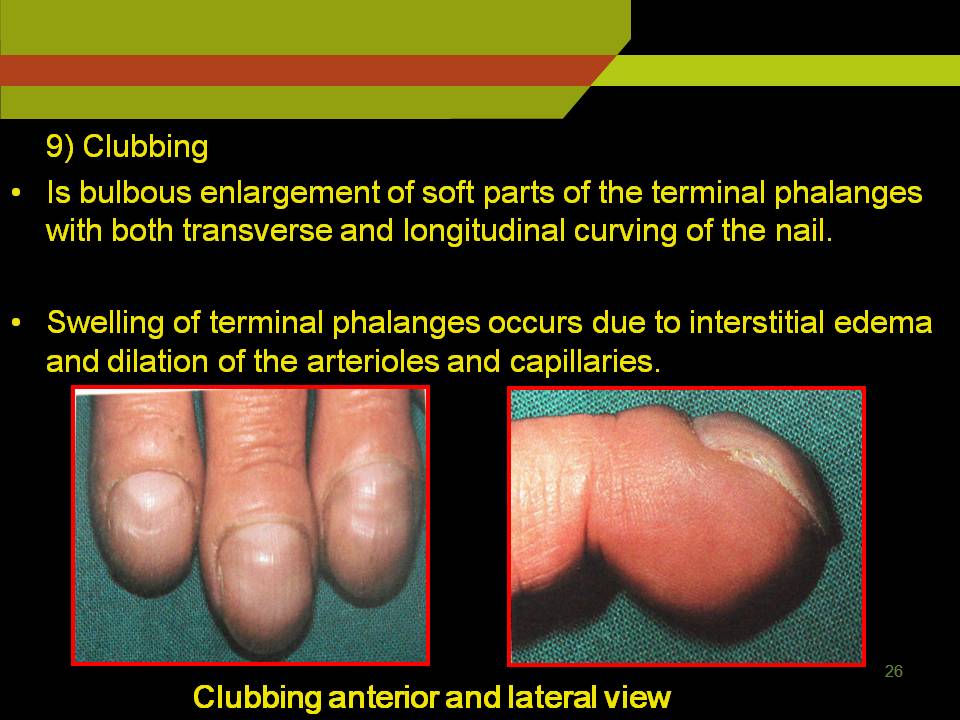
CLUBBING:
Is bulbous enlargement of soft parts of the terminal phalanges with both transverse and longitudinal curving of the nail.
Swelling of terminal phalanges occurs due to interstitial edema and dilation of the arterioles and capillaries.
Causes:
- Pulmonary: Bronchogenic carcinoma
Lung abscess
Bronchiectasis
TB with secondary infection
- Cardiac: Infective colitis
Chrons disease
Biliary cirrhosis
- Endocrine: Myxedema
Acromegaly
Grades:
Grade-I: Softening of nail bed
Grade-II: Obliteration of angle of nail bed
Grade-III: Swelling of the subcutaneous tissues over the base of the nail, causing overlying skin to become shiny, tense, and increasing curvature of nail bed, resulting in parrot beak/drum stick appearance.
Grade-IV: Swelling of fingers in all dimensions
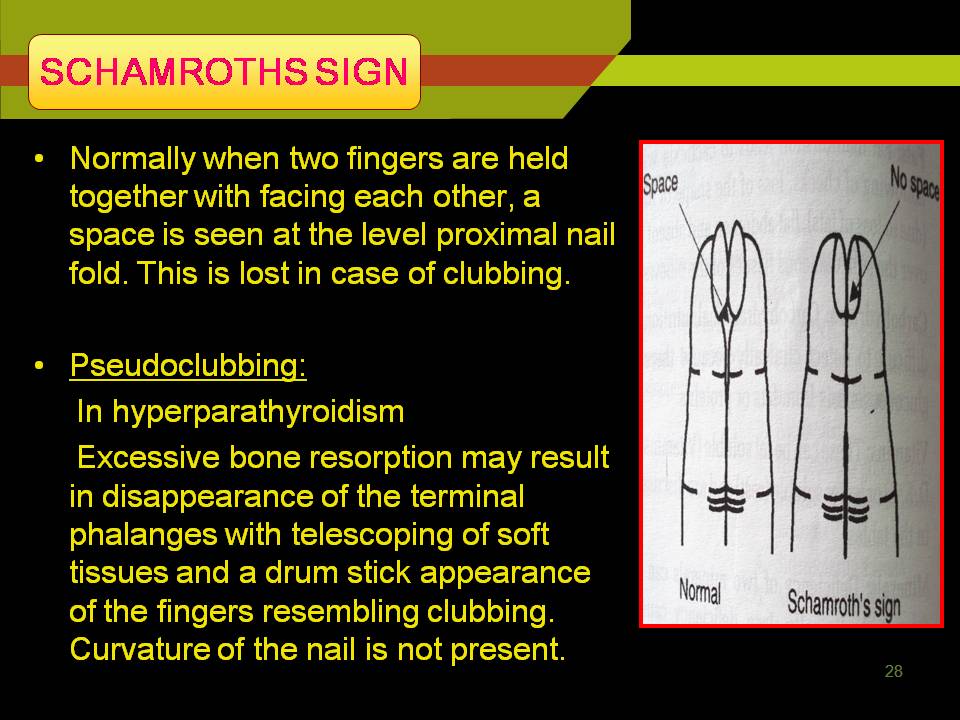
SCHAMROTHS SIGN:
Mechanism:
Exact mechanism is not known, but it believed that is due to hypoxia.
Pseudo clubbing: Seen in hyper parathyroidism.
Due to excessive bone resorption results in disappearance of the terminal phalanges with telescoping of soft tissues and drum stick appearance of the fingers— clubbing.
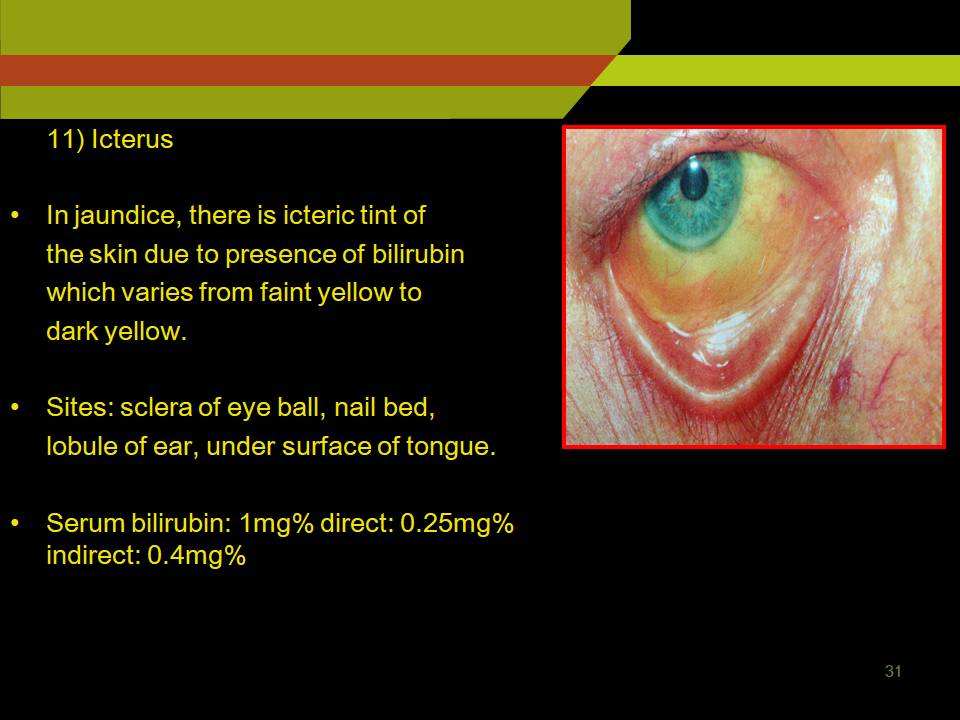
ICTERUS:
In jaundice, there is icteric tint of the skin due to presence of bilirubin which varies from faint yellow to dark yellow.
Sites: Sclera of eye ball, nail bed, lobule of ear, under surface of tongue.
Serum bilirubin: 1mg% Direct: 0.25mg%
Indirect: 0.4mg
EXTRA ORAL EXAMINATION:
1. SKIN:
a. Appearance: Rashes, Sores, Swellings or itching H/O sun exposure.
b. Color: Anemia and Jaundice
Generalized pallor: severe anemia, syncope, LVF, shock.
Pale lemon yellow tint: hemolytic jaundice
Dark yellow or orange tint: Obstructive jaundice.
c.Texture: Thickened greasy and loose in acromegaly.
Skin is atrophied with age and sometimes after treatment with glucocorticoids.
- Eruptions: Macule, papule, vesicle, and bulla.
- Pigmentation: Addisions disease (affects skin and buccal mucosa)
Vonrecklinghausens disease; coffee with milk pigmentation of limbs trunk and face.
EDEMA:
Acute nephritis; edema of face is marked when patient rises in the morning.
HEAD: Symptoms like head ache
Nature of head ache:
Unilateral/bilateral/frontal.
Persistent or intermittent and localized or generalized
Familial disorders/ induced by stress.
Following points should be asked:
Site: Location of head ache
Radiation: Does localized or spread to other places
Severity: Does it interfere with daily activities or it disturbs sleep.
Timing and duration
Character: Shooting / Piercing
Aggravating and relieving factors.
NOSE, PARA NASAL SINUSES, ALAE, EXTERNAL EAR AND NASAL MUCOSA:
Acute sinusitis: due to infection from upper teeth may drain into maxillary sinus.
Symptoms of nasal disease: Nasal obstruction, discharge, sneezing, disturbances of smell.
Long standing nasal obstruction suggests a deviated nasal septum.
Nasal discharge; purulent, bloody, watery, and mucoid.
Epistaxis (nasal bleeding)
JAWS:
Normal anatomic land marks
Any deviation in path of closure and opening lateral movements of mandible
Tenderness over the joint and muscles of mastication
Any injuries trauma to the facial bones and jaws should be examined.
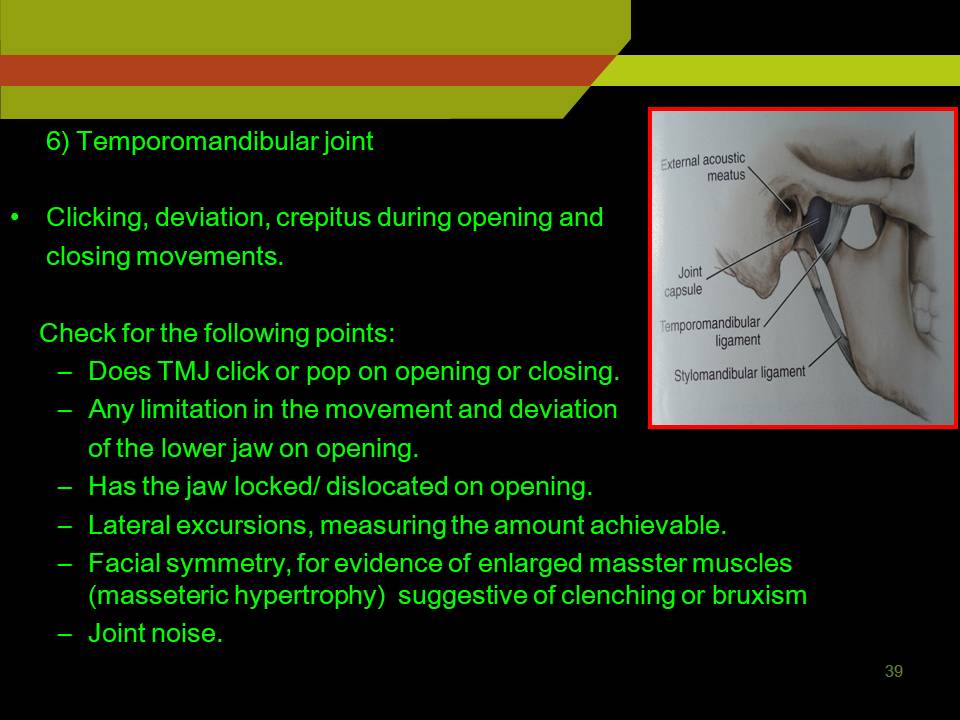
TMJ:
Clicking, deviation, crepitus during opening and closing movements.
Check for the following points:
- Does TMJ click or POP on opening or closing.
- Any limitation in the movement and deviation of the lower jaw on opening.
- Has the jaw locked/ dislocated on opening.
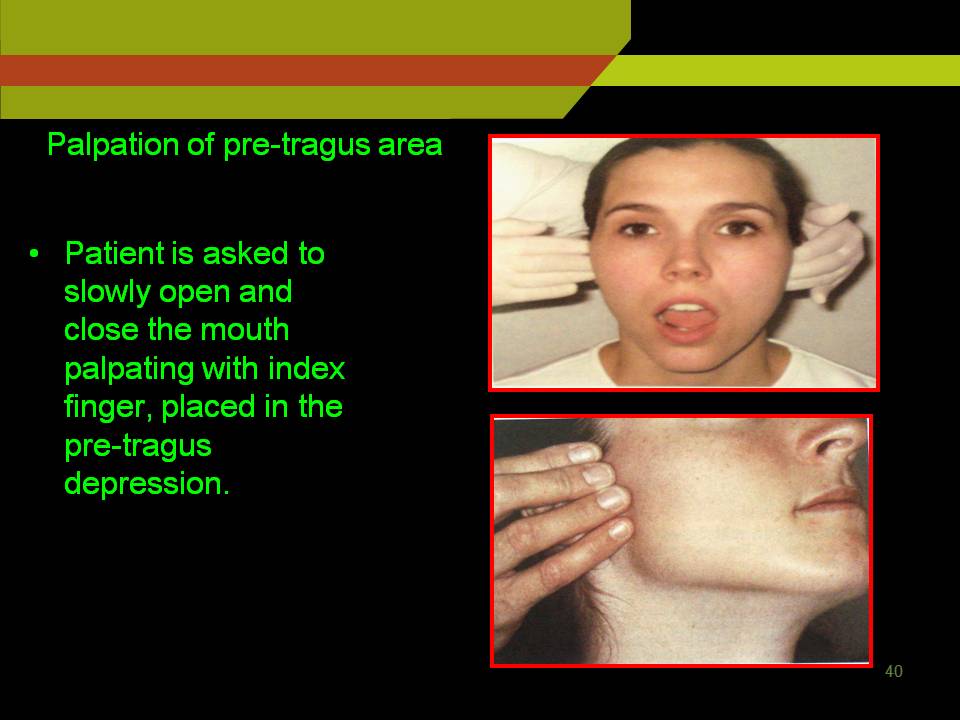
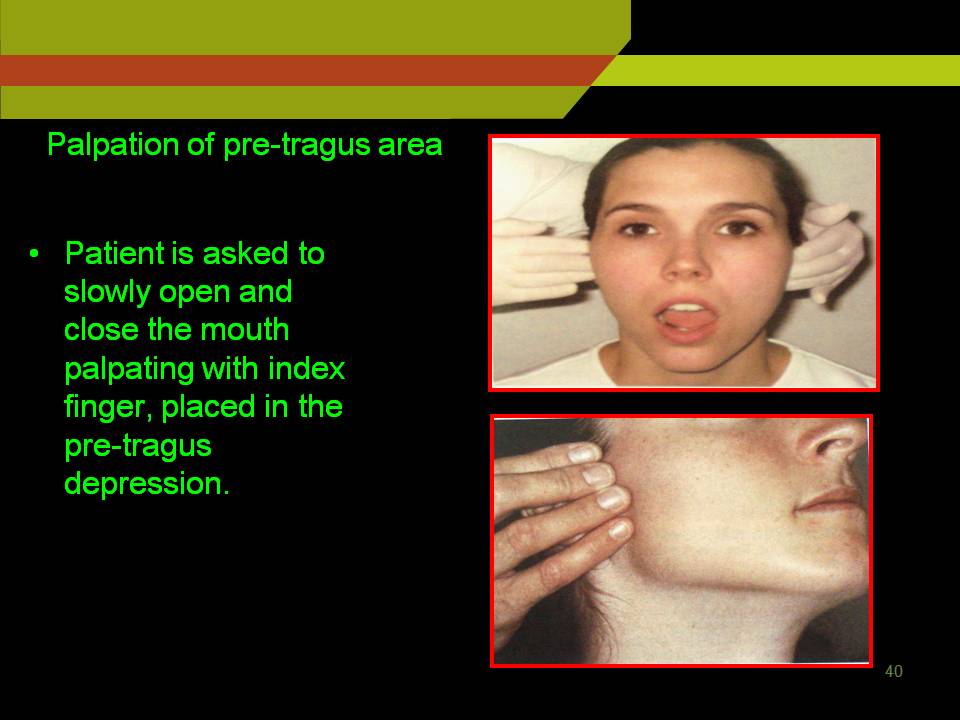
Palpation of pre tragus area:
Patient is asked to slowly open and close the mouth palpating with index finger, placed in the pre tragus depression.
Intra auricular palpation:
Performed by inserting small finger into the ear canal and pressing anteriorly.
While palpating with this methods check whether condyle moves symmetrically, with the rotation and translation phase.
Palpation is also used to detect the tenderness clicking and crepitus.

Mouth opening: Normal 35 to 50 mm
Cause for reduced mouth opening
- OSMF
- Impacted 3rd molar
- Improper techniques used in local anesthesia injections.
Muscles of mastication:
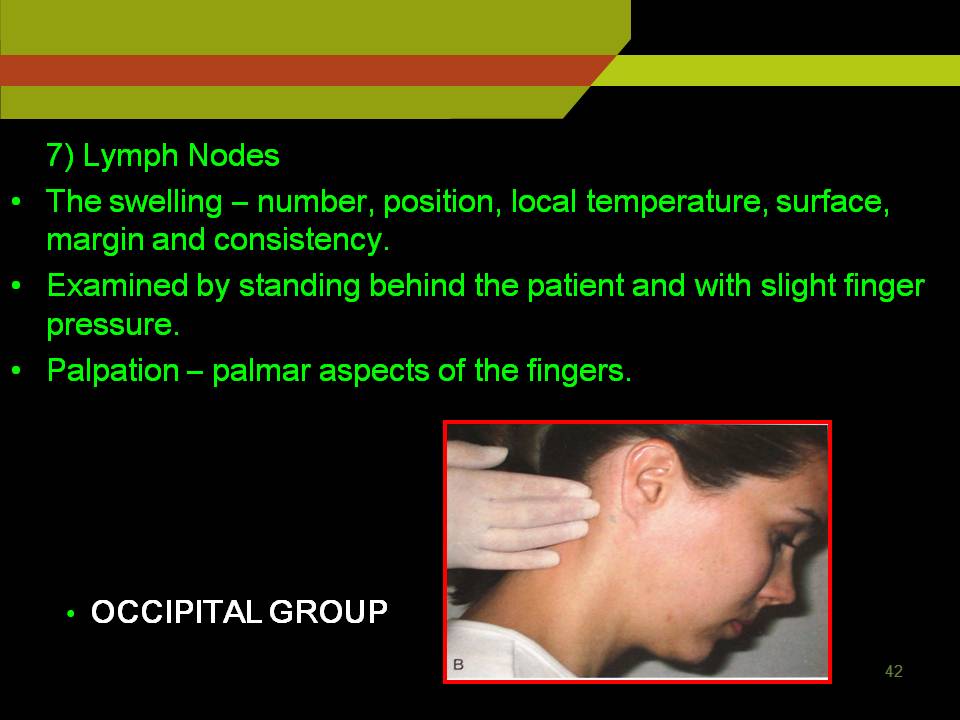
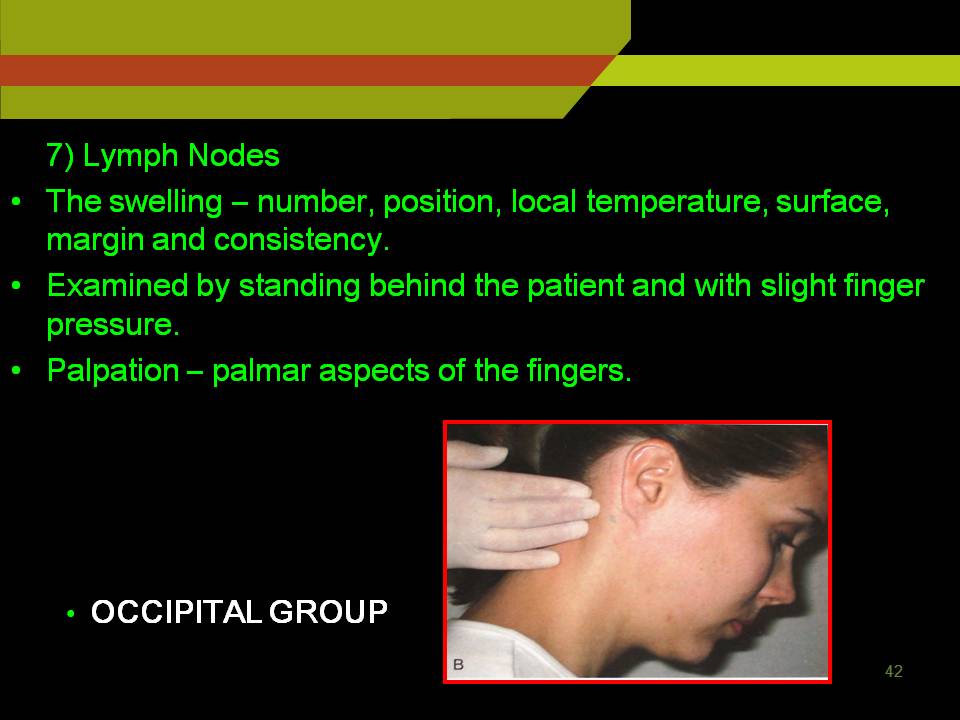
LYMPH NODE EXAMINATION:
Inspection:
Position
Number: Localized
Generalized- Hodgkin’s disease, lympho sarcoma, Lymphatic leukemia.
Palpation:
Number
Situation
Local temperature
Surface, margin, and consistency
Enlarged lymph node are palpated with palmer aspect of fingers
While rolling the fingers against swelling slight pressure is maintained to know actual consistency
Fixity to underlying tissues: E.g. Malignancy.
Palpation of LN begins with most superior nodes and worked down the clavicle for supraclavicular.
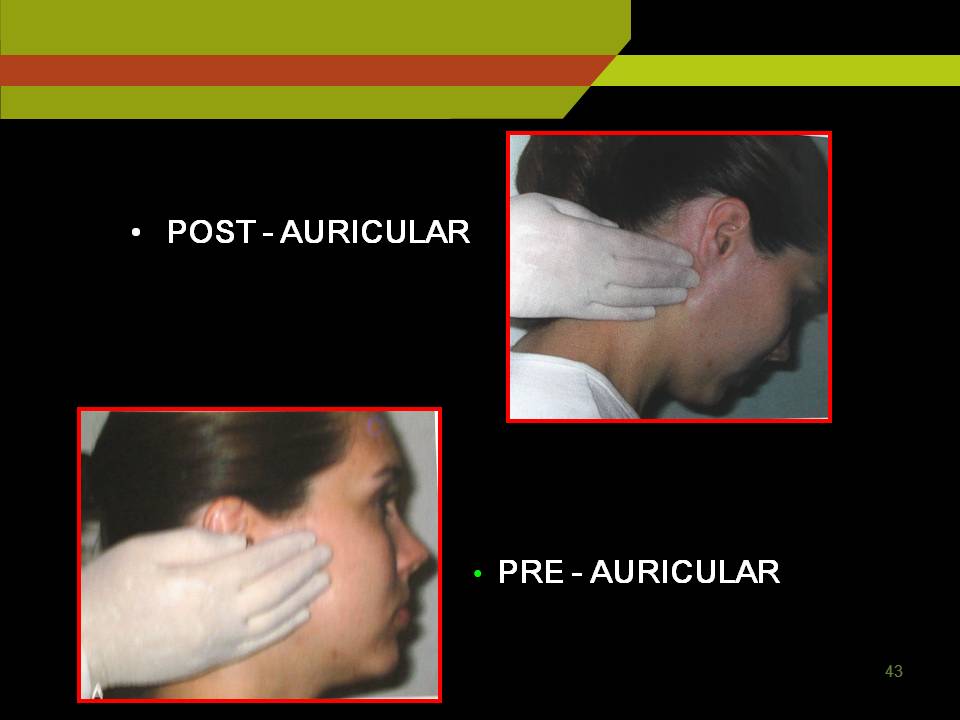
Pre auricular nodes: anterior to tragus of ear
Post auricular and occipital nodes: In mastoid and base of the skull
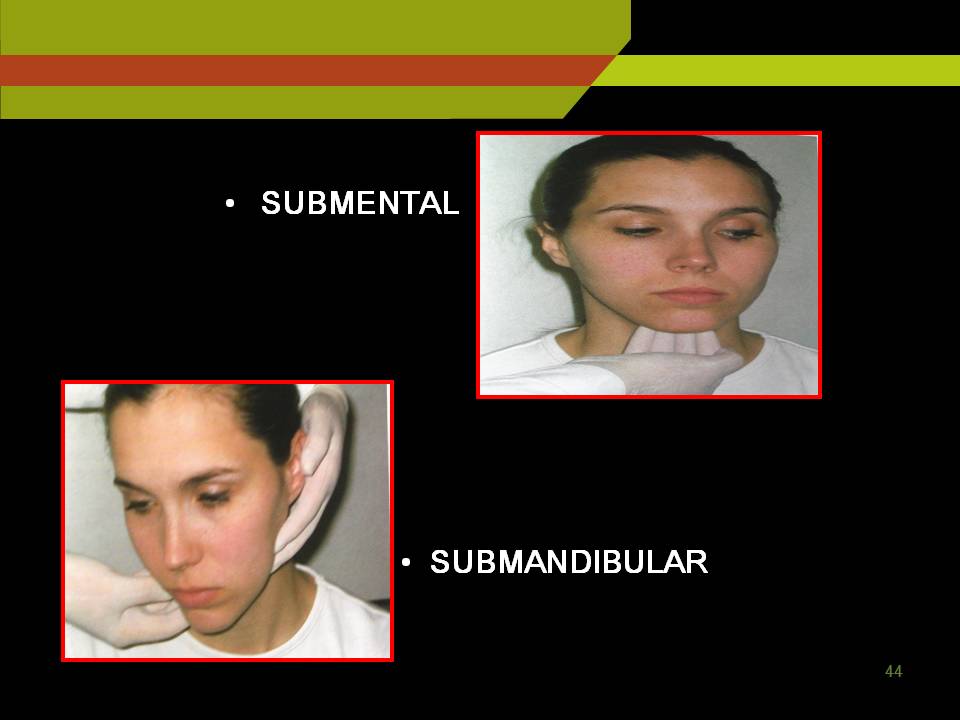
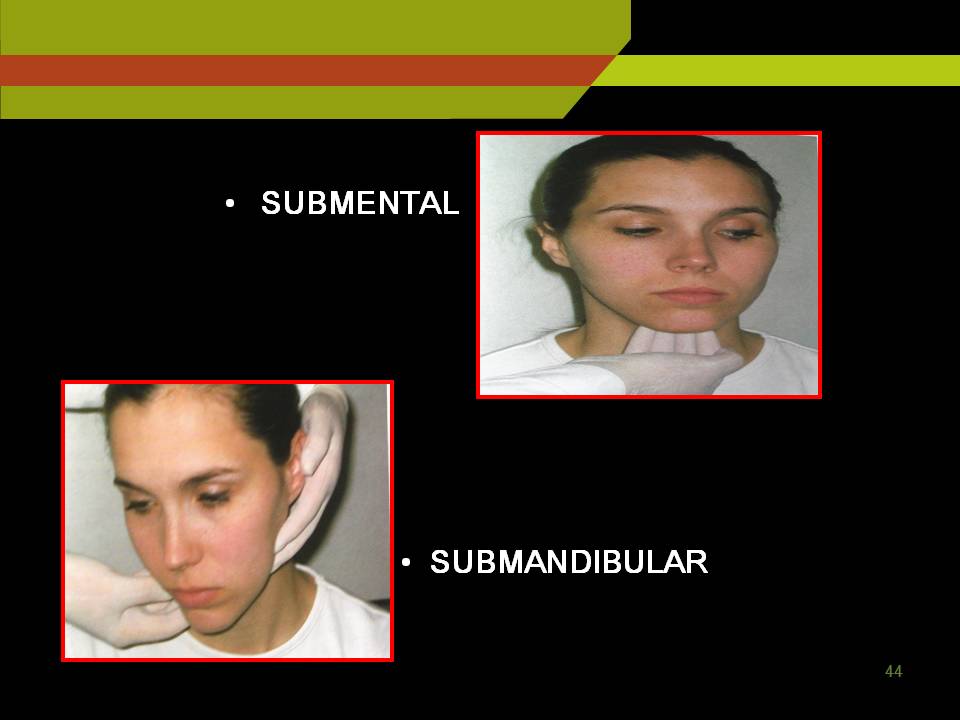
Sub mental nodes: Under the chin further posteriorly sub mandibular and sub lingual LN.
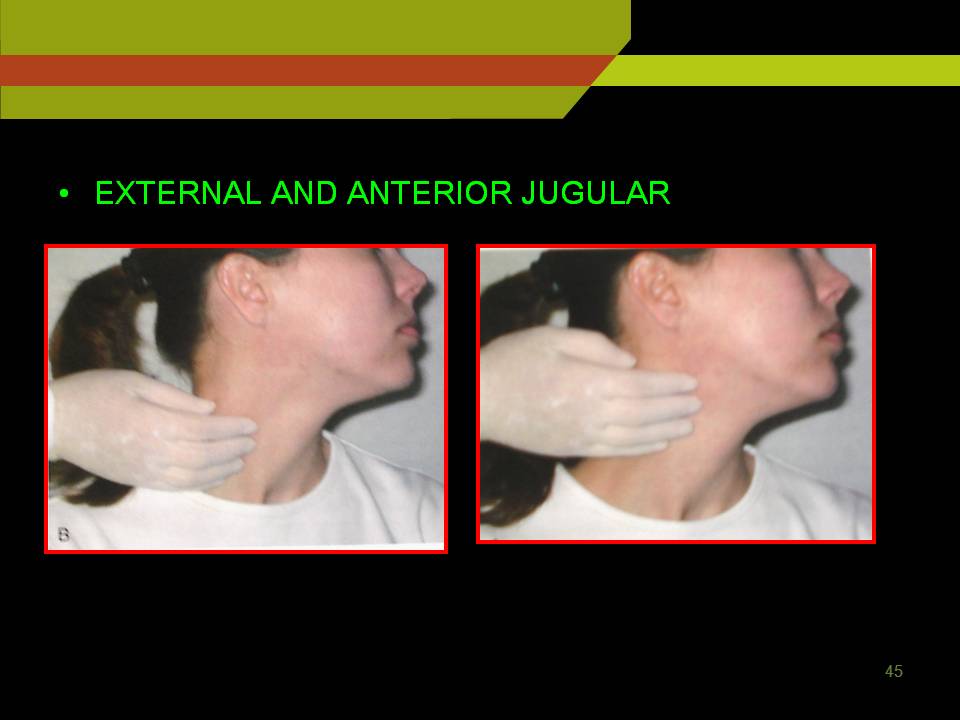
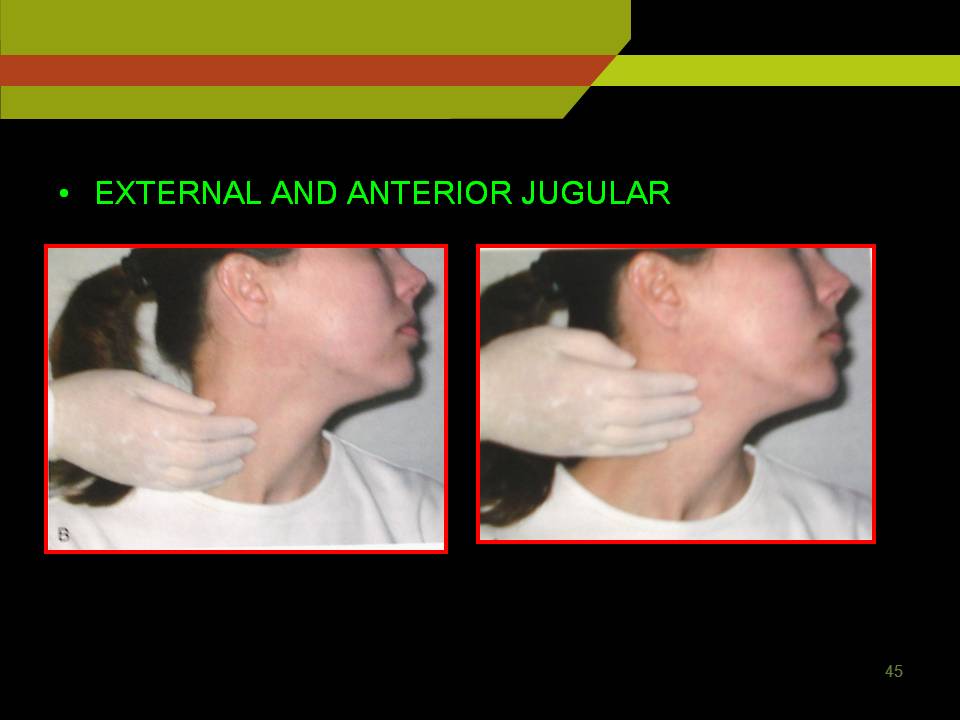
To examine deep cervical lymph nodes:
Ask the patient to sit erect and turn the head to one side to relax the sternocleidomastoid muscle use thumb and index finger to palpate under the anterior and posterior borders of the relaxed muscle and repeat the procedure on opposite side.
Posterior cervical nodes are palpated in posterior triangle close to anterior border of the trapezius muscle finally check for supraclavicular LN just above the clavicle, lateral to the attachment of sternocleidomastoid.
Normal LN is difficult to palpate
Nodes draining area of active infection are usually tender overlying skin warm and red.
LN enlarged in absence of local infection suggests systemic infection (infectious mononucleosis, HIV infection)
INTRA-ORAL EXAMINATIONS
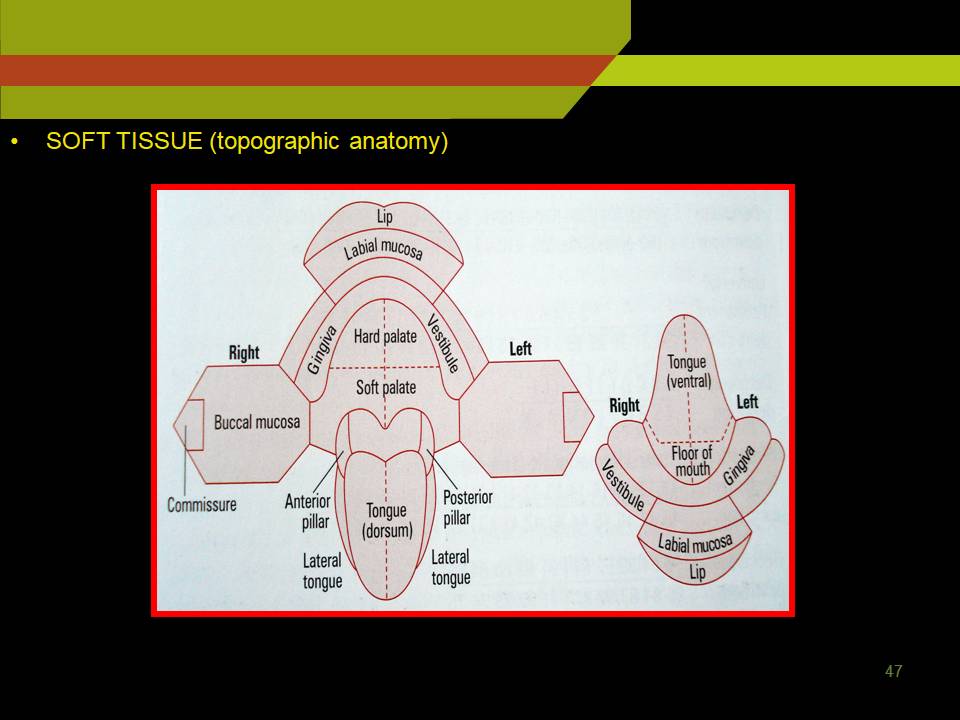
SOFT TISSUE
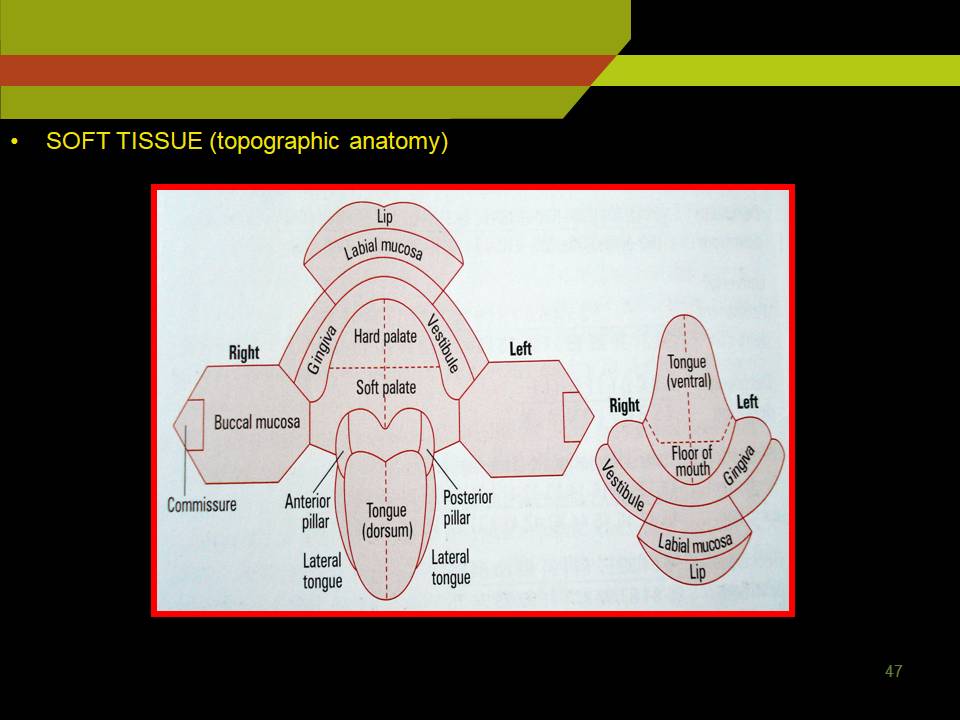
Soft Tissue (topographic anatomy)
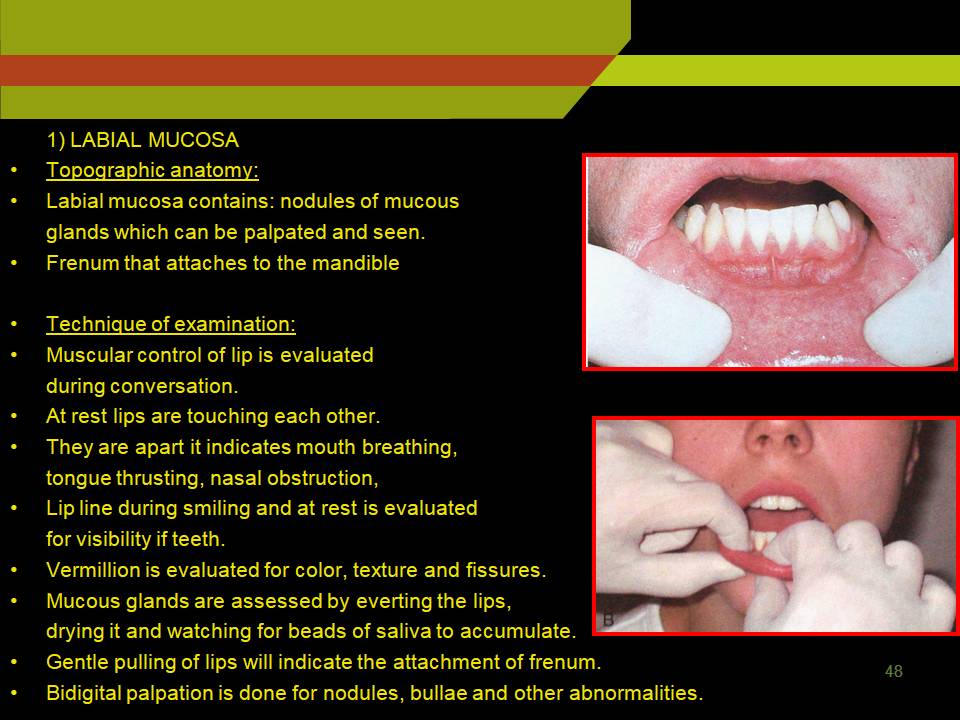
1) LABIAL MUCOSA
Labial mucosa contains: nodules of mucous glands which can be palpated and seen.
Frenum that attaches to the mandible
Technique of examination:
Muscular control of lip is evaluated during conversation.
At rest lips are touching each other.
They are apart it indicates mouth breathing, tongue thrusting, nasal obstruction,
Lip line during smiling and at rest is evaluated for visibility if teeth.
Vermillion is evaluated for color, texture and fissures.
Mucous glands are assessed by everting the lips, drying it and watching for beads of saliva to accumulate.
Gentle pulling of lips will indicate the attachment of frenum.
Bidigital palpation is done for nodules, bullae and other abnormalities.
Labial Mucosa Palpation
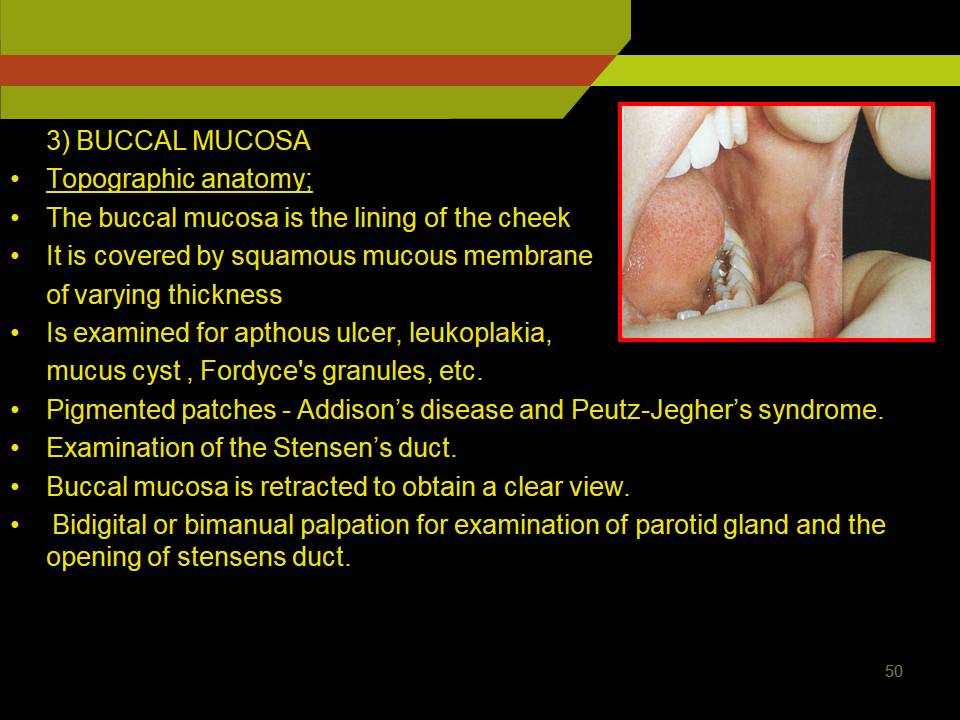
2) BUCCAL MUCOSA
Topographic anatomy;
The buccal mucosa is the lining of the cheek
It is covered by squamous mucous membrane of varying thickness
Is examined for apthous ulcer, leukoplakia, mucus cyst , Fordyce’s granules, etc.
Pigmented patches – Addison’s disease and Peutz-Jegher’s syndrome.
Examination of the Stensen’s duct.
Buccal mucosa is retracted to obtain a clear view.
Bidigital or bimanual palpation for examination of parotid gland and the opening of stensens duct.
Buccal Mucosa Palpation
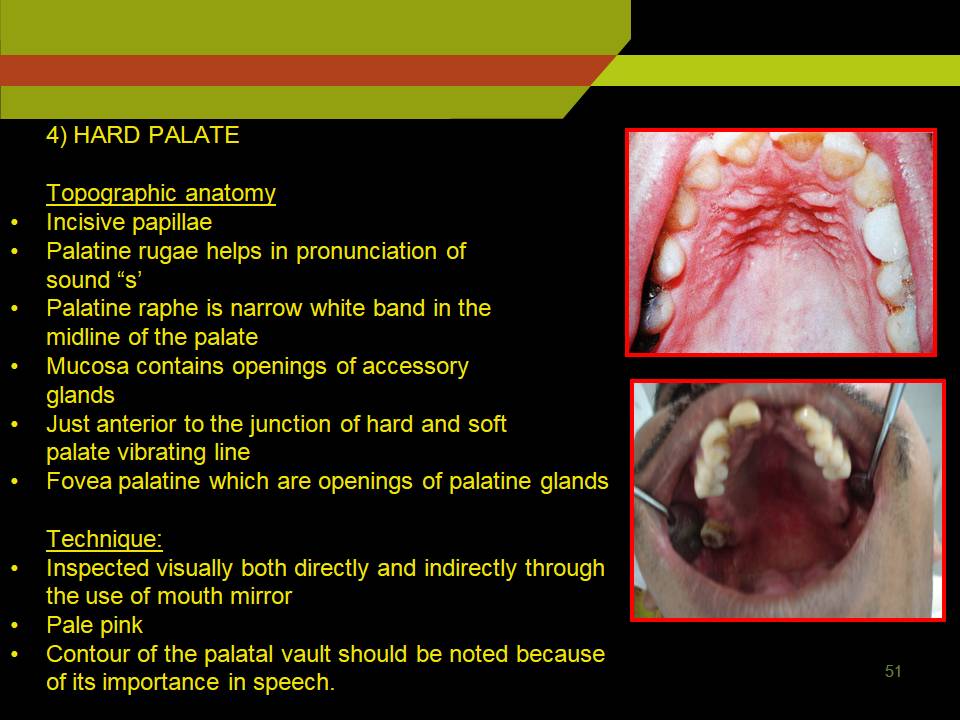
3) HARD PALATE
Topographic anatomy
Incisive papillae
Palatine rugae helps in pronunciation of sound “s’
Palatine raphe is narrow white band in the midline of the palate
Mucosa contains openings of accessory glands.
Just anterior to the junction of hard and soft palate vibrating line
Fovea palatine which are openings of palatine glands
Technique:
Inspected visually both directly and indirectly through the use of mouth mirror.
Pale pink
Contour of the palatal vault should be noted because of its importance in speech.
Hard Palate
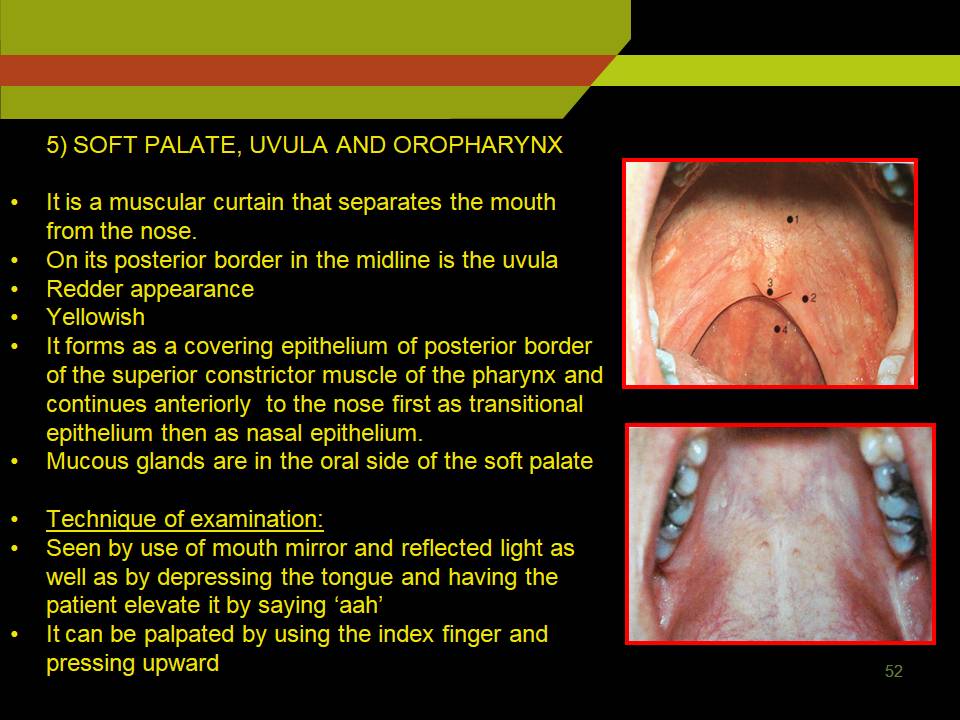
4) SOFT PALATE, UVULA AND OROPHARYNX
It is a muscular curtain that separates the mouth from the nose.
On its posterior border in the midline is the uvula
Redder appearance
Yellowish
It forms as a covering epithelium of posterior border of the superior constrictor muscle of the pharynx and continues anteriorly to the nose first as transitional epithelium then as nasal epithelium.
Mucous glands are in the oral side of the soft palate
Technique of examination:
Seen by use of mouth mirror and reflected light as well as by depressing the tongue and having the patient elevate it by saying ‘aah’.
It can be palpated by using the index finger and pressing upward.
Soft Palate
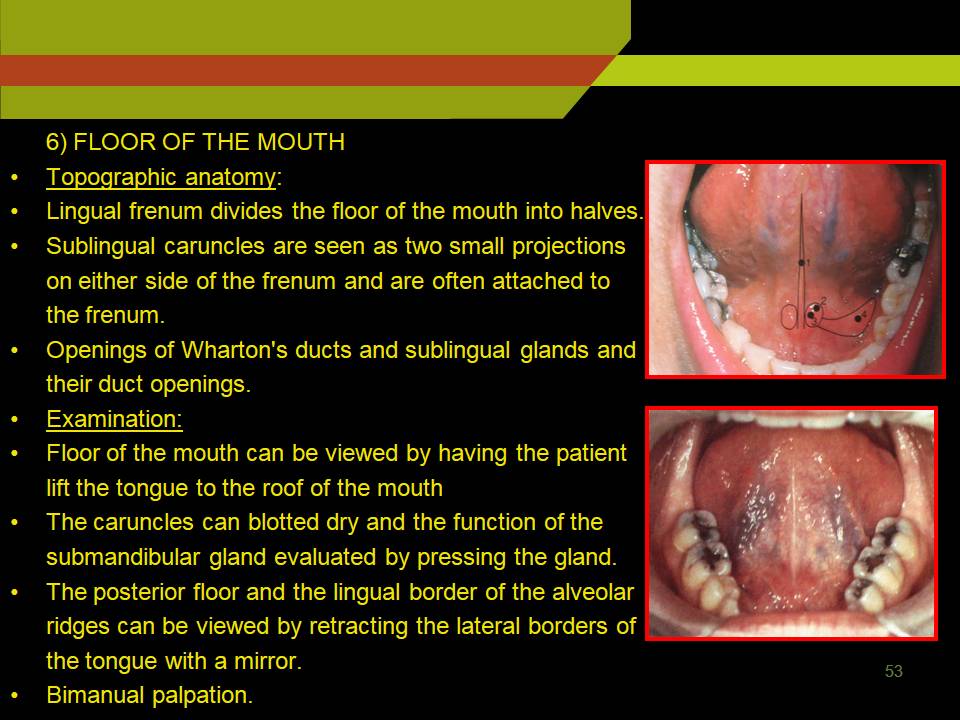
5) FLOOR OF THE MOUTH
- Topographic anatomy:
- Lingual frenum divides the floor of the mouth into halves.
- Sublingual caruncles are seen as two small projections on either side of the frenum and are often attached to the frenum.
- Openings of Wharton’s ducts and sublingual glands and their duct openings.
Examination:
- Floor of the mouth can be viewed by having the patient lift the tongue to the roof of the mouth
- The caruncles can blotted dry and the function of the submandibular gland evaluated by pressing the gland.
- The posterior floor and the lingual border of the alveolar ridges can be viewed by retracting the lateral borders of the tongue with a mirror.
- Bimanual palpation.
Flour of Mouth
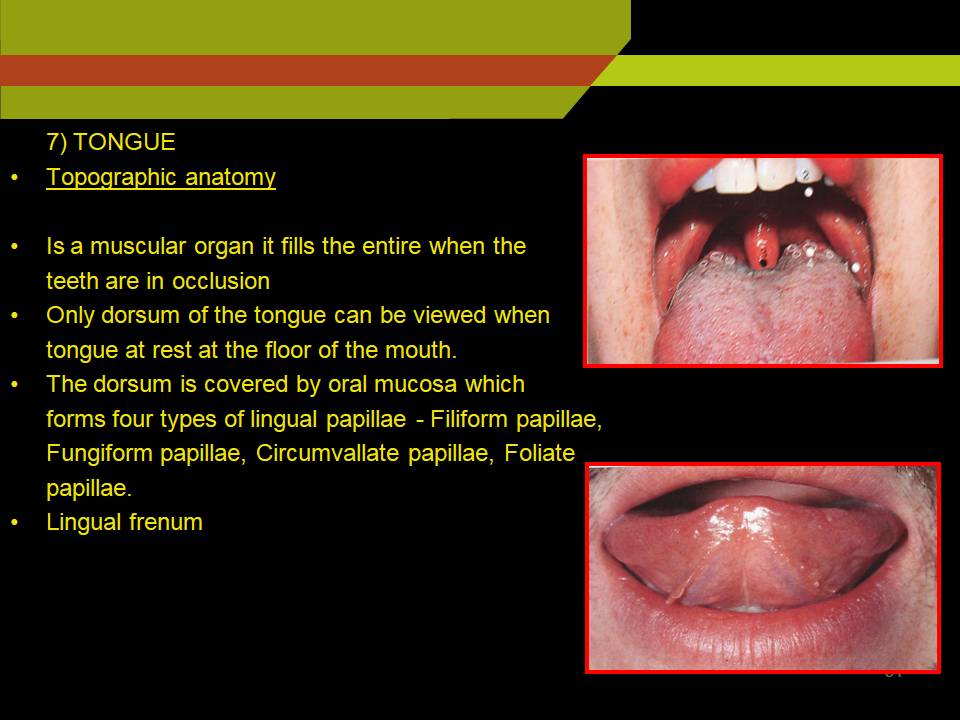
6) TONGUE
- Topographic anatomy
- Is a muscular organ it fills the entire when the teeth are in occlusion
- Only dorsum of the tongue can be viewed when tongue at rest at the floor of the mouth.
- The dorsum is covered by oral mucosa which forms four types of lingual papillae – Filiform papillae, Fungiform papillae, Circumvallate papillae, Foliate papillae.
- Lingual frenum
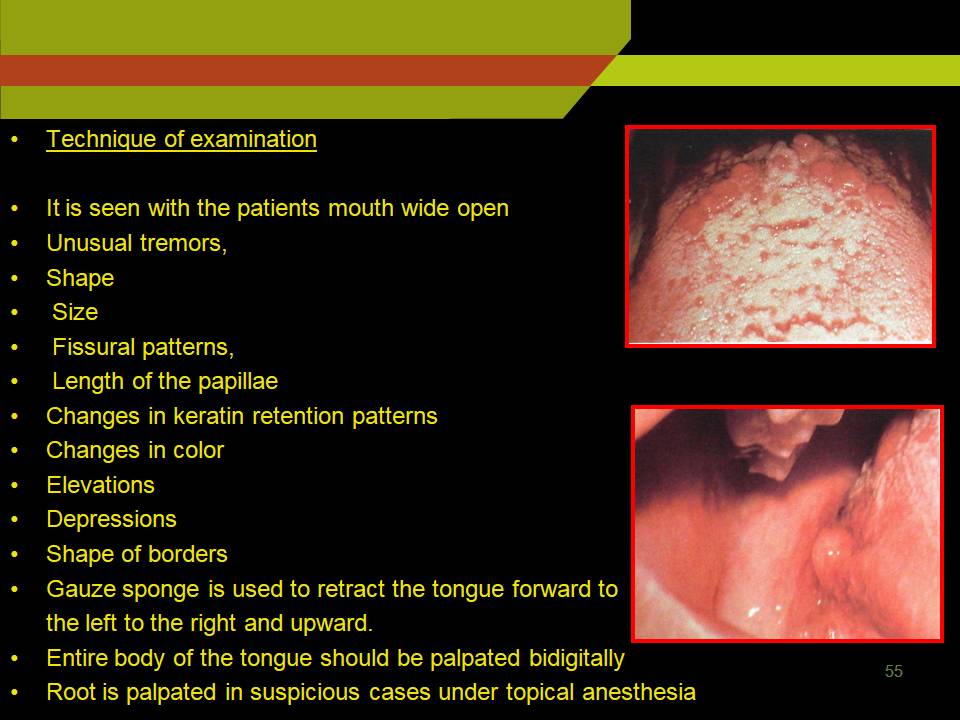
Technique of examination
- It is seen with the patients mouth wide open
- Unusual tremors,
- Shape
- Size
- Fissural patterns,
- Length of the papillae
- Changes in keratin retention patterns
- Changes in color
- Elevations
- Depressions
- Shape of borders
- Gauze sponge is used to retract the tongue forward to the left to the right and upward.
- Entire body of the tongue should be palpated bidigitally.
- Root is palpated in suspicious cases under topical anesthesia.
Tongue
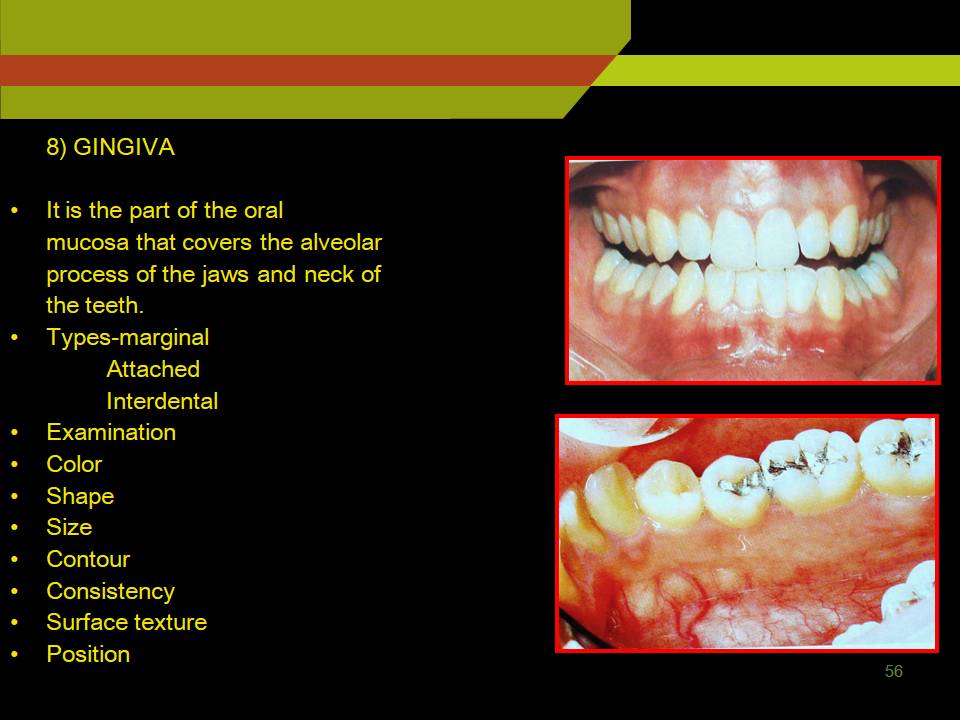
7) GINGIVA
- It is the part of the oral mucosa that covers the alveolar process of the jaws and neck of the teeth.
- Types-marginal
Attached
Interdental
- Examination
- Color
- Shape
- Size
- Contour
- Consistency
- Surface texture
- Position
8) PERIODONTAL LIGAMENT
- The PDL is the connective tissue that surrounds the root and connects with the bone
- Periodontal fibers
- Transseptal
- Alveolar crest
- Horizontal
- Oblique
- Apical
- Interradicular
- Recession
- Is exposure of root surface by an apical shift in the position of the gingiva
- Types-
- Visible-clinically observable
- Hidden-covered by gingiva
- Causes
- Faulty tooth brushing
- Tooth malposition
- High frenal attachment
- Trauma from occlusion
9) SALIVARY GLANDS
- Major salivary glands should be inspected and palpated for
- Facial symmetry
- Evidence of enlarged glands
- Evidence of salivary flow from salivary ducts
- Saliva appearance
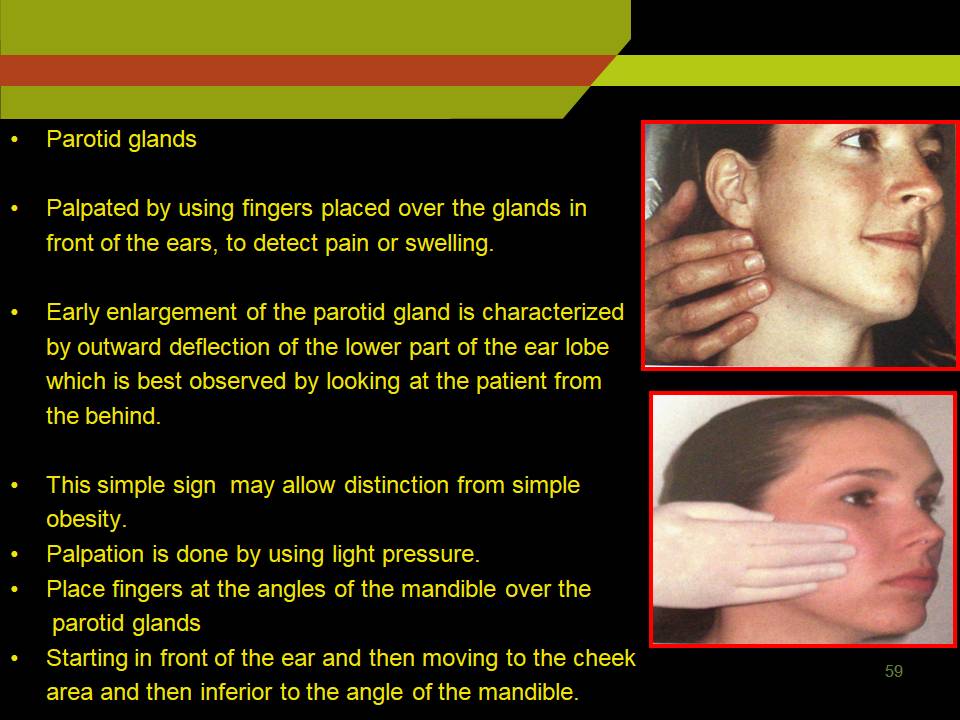
PAROTID GLANDS
- Palpated by using fingers placed over the glands in front of the ears, to detect pain or swelling.
- Early enlargement of the parotid gland is characterized by outward deflection of the lower part of the ear lobe which is best observed by looking at the patient from the behind.
- This simple sign may allow distinction from simple obesity.
- Palpation is done by using light pressure.
- Place fingers at the angles of the mandible over the parotid glands
- Starting in front of the ear and then moving to the cheek area and then inferior to the angle of the mandible.
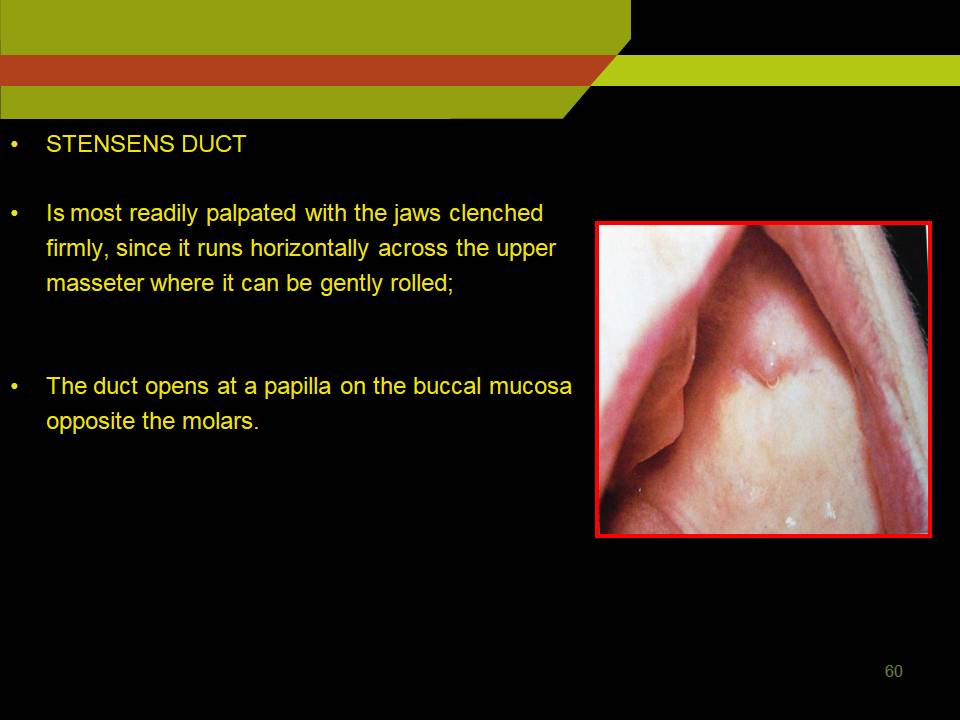
STENSENS DUCT
- Is most readily palpated with the jaws clenched firmly, since it runs horizontally across the upper masseter where it can be gently rolled;
- The duct opens at a papilla on the buccal mucosa opposite the molars.
Stensens Duct
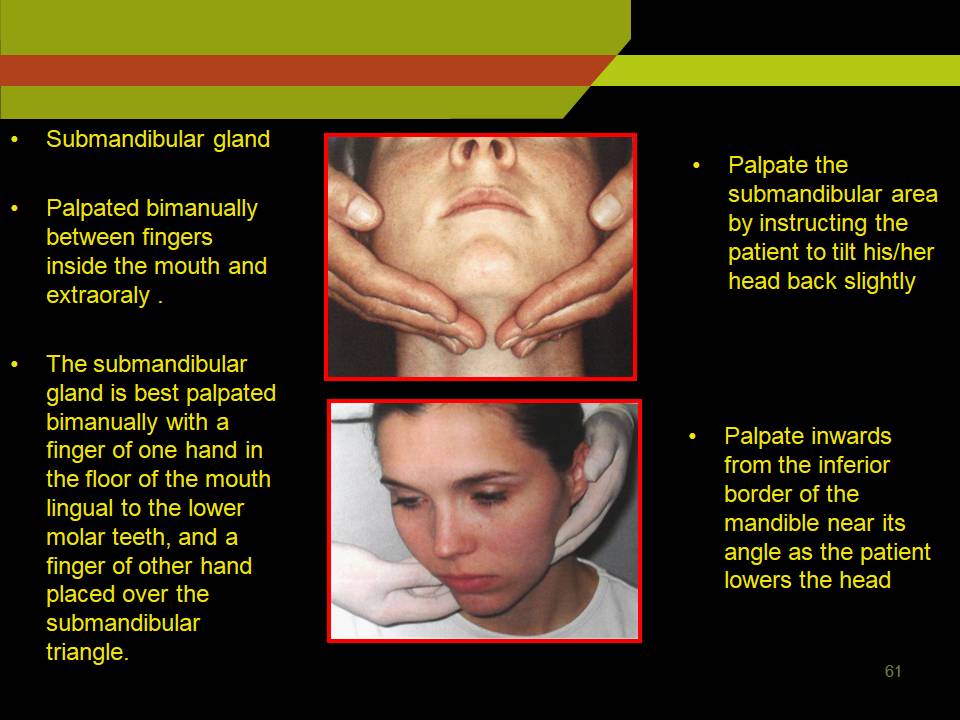
SUBMANDIBULAR GLAND
- Palpated bimanually between fingers inside the mouth and extraoraly .
- The submandibular gland is best palpated bimanually with a finger of one hand in the floor of the mouth lingual to the lower molar teeth, and a finger of other hand placed over the submandibular triangle.
- Palpate the submandibular area by instructing the patient to tilt his/her head back slightly
- Palpate inwards from the inferior border of the mandible near its angle as the patient lowers the head
Submandibular gland.
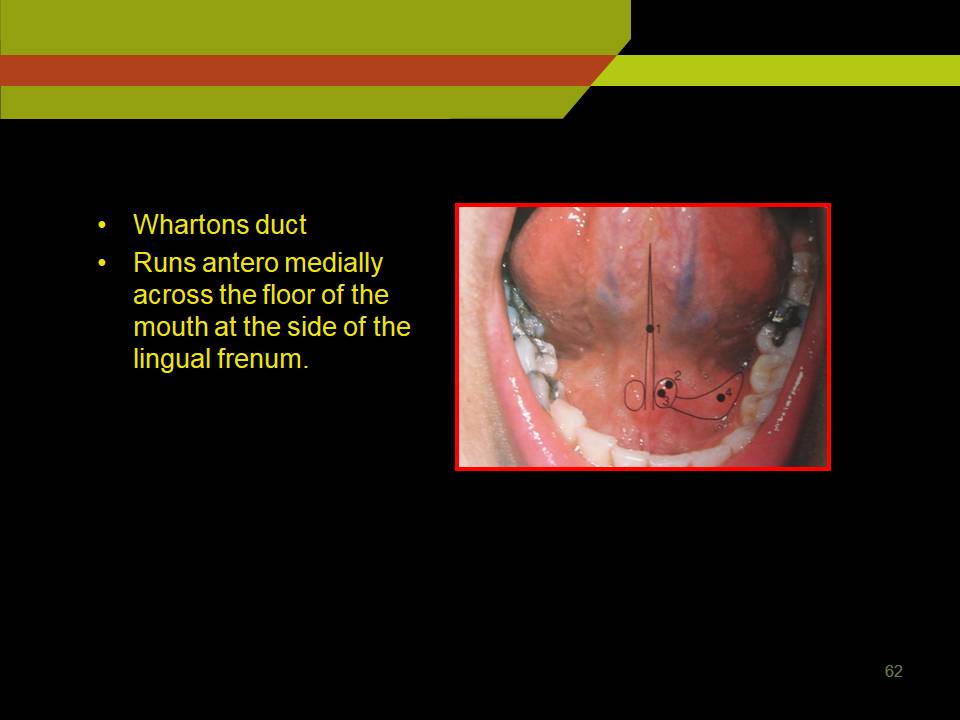
- Whartons duct
- Runs antero medially across the floor of the mouth at the side of the lingual frenum.
Whartons Duct
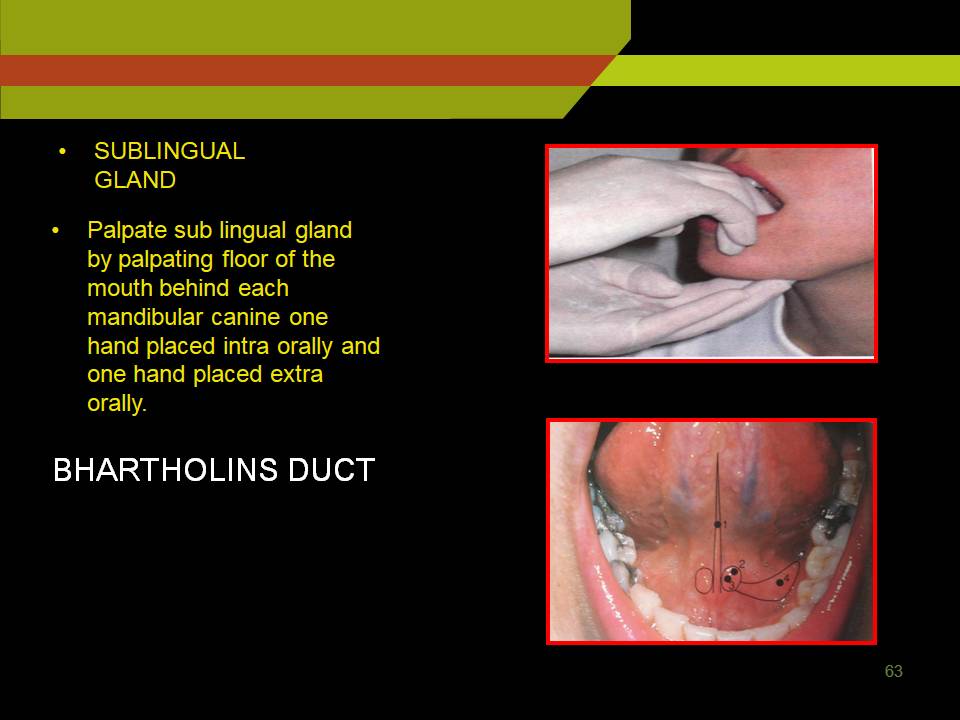
- SUBLINGUAL GLAND
- Palpate sub lingual gland by palpating floor of the mouth behind each mandibular canine one hand placed intra orally and one hand placed extra orally.
HARD TISSUES
1) Teeth Present
- Primary
- Mixed
- Permanent
2) Teeth Nomenclature
- Zsingmondy and Palmar method
- Universal system
- FDI (two digit system)
3) Dental caries ( pit and fissures, smooth surface or cervical caries)
4) Recurrent caries
5) Missing teeth
6) Wearing diseases
a) Attrition: physiologic wearing away of a tooth as a result of tooth to tooth contact, as in mastication.
- Site: occlusal, incisal and proximal surfaces of teeth.
- Etiology: bruxisum, traumatic occlusion, and associated with aging process.
b) Abrasion: pathological wearing away of tooth substance due to some abnormal mechanical process.
- Occurs on the exposed surfaces of teeth, although sometimes occurs on incisal or proximal surfaces.
- Etiology: use of abrasive dentifrice, tooth floss, tooth picks and in tailors who as habit of opening bobby pins with the teeth.
c) Erosion
- Defined as irreversible loss of dental hard tissue by a chemical process that does not involve bacterial process.
- Site: cervical areas of teeth.
- Etiology: intrinsic, due to gastro esophageal reflux and vomiting
- Extrinsic: acidic beverages, citrus fruits.
d) Abfraction: pathologic loss of both enamel and dentin caused by biomechanical loading forces.
- Site: cervical areas closely resemble erosion or abrasion
- Clues to diagnose: defects that are deep narrow and V-shaped do not allow the tooth brush to contact the base of the defect, and often affect single tooth with adjacent unaffected teeth.
- Seen exclusively on the facial surface and exhibit much prevalence in those with bruxism
- More commonly seen in mandibular teeth because of their lingual orientation makes them susceptible to concentration of the tensile stresses at the cervical region.
7) Mobility of teeth
- To evaluate the integrity of the attachment apparatus surrounding the teeth.
Types:
a) Pathologic mobility: it results from inflammatory process, para functional habits.
b) Adaptive mobility: occurs due to anatomic factors such as short roots or poor crown to root ratio.
Scores of mobility: (given by Millar in 1950)
0 – no detectable movement when force is applied other than what is considered normal
(physiologic) motion.
1 – mobility greater than normal.
2 – mobility of tooth about 1mm in bucco-lingual direction.
3 – mobility of tooth more than 1mm in bucco-lingual direction and labio-palatal
direction combined with depression of tooth in the socket.
8) Occlusion
Angles classification
Class-I molar relation: mesio-buccal cusp of the maxillary 1st molar occludes in the buccal groove of mandibular 1st permanent molar.
Dewey’s modification: Type I – Type V.
Class-II: distobuccal cusp of upper first molar occludes in the buccal groove of lower first permanent molar.
- Division-I: proclination of upper incisors abnormal muscular activity.
- Division-II: lingual inclined upper central incisors and labially tipped upper lateral incisors overlying the central incisors.
- Sub division-II: class-II molar relationship on one side and class-i on the other side
Class-III: mesiobuccal cusp of maxillary first permanent molar occludes in interdental space between mandibular first second molar.
9) Discoloration or staining
- Pigmented deposits on the tooth surface are called stains
Extrinsic:
Bacterial stains
Iron
Tobacco
Foods and beverages
Gingival hemorrhage
Restorative materials
Medications
Intrinsic:
Amelogenesis imperfecta
Dentinogenesis imperfecta
Dental fluorosis
Erythropoietic porphyria
Hyperbilirubinemia
Onchronosis
Trauma
Localized red blood cell break down
Medications
10) Periodontal pocket
- True pocket
- False pocket
- Probe inserted parallel to vertical axis of the tooth and walked around each surface of each tooth.
- Furcation involvement – it is the invasion of the bifurcation and trifurcation of the multi-rooted teeth by the periodontal disease.
- Grades:
Grade I – it is incipient bone loss.
Grade II – partial bone loss
Grade III – total bone loss with through and through opening of the furcation.
Grade IV – Grade III + gingival recession.
PROVISIONAL/ TENTATIVE DIAGNOSIS
It refers to a preliminary educated guess as to the nature of a condition before all diagnostic data are assembled.
DIFFERENTIAL DIAGNOSIS
It refers to the process of identifying a disease or a condition by differentiating it from all other pathological process that have similar symptoms.
LABORATORY INVESTIGATIONS
They help to come to the final diagnosis eg. In case of proximal caries, the provisional diagnosis will be mesial or distal caries. Radiograph will confirm the diagnosis and help to differentiate into incipient, moderate, advanced and severe caries.
Methods of investigation
- Hematological investigations
- Urine analysis
- Biochemical investigation
- Radiological investigations
- Histopathological investigations
- Microbiological investigations
- Special investigations like Sialography, MRI, etc.
FINAL DIAGNOSIS
It is the diagnosis arrived at after all the data obtained from history, physical examination and laboratory studies are collected, analyzed and subjected to logical thinking.
It usually identifies the diagnosis for the patient’s chief complaint first, with subsidiary diagnosis of concurrent problems.
TREATMENT PLANNING
Emergency Phase
Promotive Phase
Curative Phase
Rehabilitative Phase
CONCLUSION
- History taking is not only science but is a real art, which need practice, finish, concentration and aptitude.
- A patient comes to doctor with lot of hopes, our aim should be, to get as much information from him as possible.
- Apart from information, it is vital for doctor-patient relationship, which builds up from the first conversation.
- The history and physical examination continues, from the time the patient enters the consultation room, till he leaves it.
- Proper interpretation of the symptoms, signs and investigation, is a must for proper diagnosis.
BIBLIOGRAPHY
- Textbook of Oral Medicine by Pramod John R..
- Textbook of Oral Medicine by Anil Govindrao Ghom.
- Oral Diagnosis. The Clinician’s Guide by Warren and Stephen.



Leave a comment